Indications for use
It is important for parents to understand the main thing: an antibiotic is not a harmless and miracle pill that can be used with or without reason. Antibacterials are strong medicines, many of which can be harmful to infants. Self-prescription of a drug is unacceptable, so only a doctor can prescribe this or that medicine for you.
Severe infections sometimes require immediate treatment and the use of the fastest and most effective measures. Then antibiotics come to the rescue. We list some cases and symptoms in which antibiotics may be prescribed to a baby under one year of age:
- prolonged fever;
- severe forms of infectious diseases;
- deterioration of the patient's condition after prolonged treatment;
- purulent discharge;
- change in blood composition.
The main rule for prescribing antibiotics for a child under one year of age is this: when prescribing a medicine, the doctor must draw the correct conclusion and weigh the benefits and harms of taking certain medications. By the way, this applies not only to antibiotics, but also to any medications prescribed at such a tender age.
Among the most common antibiotics for children:
- "Amoxicillin";
- "Augmentin";
- "Zinacef";
- "Zinnat";
- "Sumamed Forte";
- "Suprax";
- "Ceftriaxone" and others.
“We had a high temperature, about 40, we didn’t know the reason, but the temperature didn’t drop for three days. They put me in the infectious diseases department, put me on a drip, and gave me the antibiotic Pantsev. The temperature subsided and the baby began to have loose stools.
As it later became clear, the cause of everything was teeth. They erupted within two weeks. The baby developed an allergy to this antibiotic: swelling of the face, rash, itching. But everything worked out, we were cured. And this was the temperature for every tooth that erupted, and I already used Amoxicillin when I couldn’t bring down the temperature for a very long time. We took antibiotics along with Linex. And everything was fine."
Happy mother Alena Larionova
Antibiotics for children with colds
Respiratory infections
On average, about 80–90% of acute respiratory infections are caused by viruses and only 5 to 10% of them are caused by bacteria and require antibacterial treatment. In most cases, acute respiratory diseases are caused by viruses. The disease occurs with a runny nose, cough and elevated body temperature. In uncomplicated cases of ARVI, antibiotics are not prescribed to children.
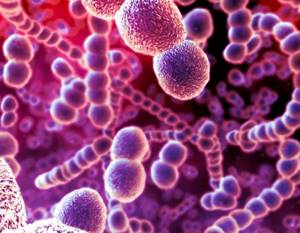
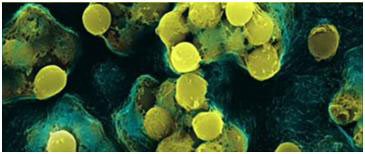
Of the bacterial flora of the upper respiratory tract, the most common are pneumococci (Fig. 2), staphylococci (Fig. 3) and streptococci (Fig. 4).
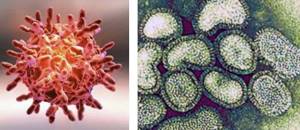
Rice. 1. Photo of the virus.
Rice. 2. Pneumococci (Streptococcus pneumoniae).
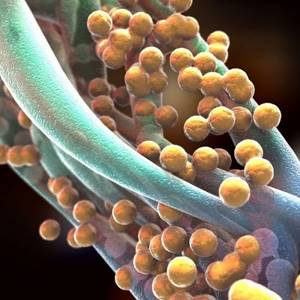
Rice. 3. Staphylococcus aureus (Staphylococcus aureus).
These “bunches of grapes” cause everything from mild skin diseases to pneumonia and sepsis.
Rice. 4. Streptococci under a microscope.
Rhinitis with mucopurulent discharge
Antibacterial drugs are prescribed only if there is a high probability of developing sinusitis.
Pharyngitis
About 80% of all pharyngitis are viral in nature and are recorded together with rhinitis, laryngitis, tracheitis and bronchitis. Antibiotics in this case are prescribed only if there is a high probability of infection with group A b-hemolytic streptococcus.

Rice. 5. The figure shows the differences between viral and bacterial tonsillitis caused by streptococcal infection.
Cough
Cough very often accompanies acute respiratory infections and bronchitis. Antibiotics for children with cough are prescribed if the disease is caused by the causative agent of whooping cough, mycoplasma or streptococcus pneumoniae. More than 90% of acute bronchitis is caused by viruses.
Persistent cough
Accompanies laryngitis, tracheitis and bronchitis. More than 90% of bronchitis is viral in nature. If the cough lasts more than 14 days, and there were symptoms of acute respiratory infections, but are no longer present, antibiotics are not indicated. It is necessary to exclude tuberculosis, etc.
A condition in which there is only an increase in temperature
Antibiotics are prescribed in 50% of cases.
Contraindications
There are a number of contraindications that your child may have that may mean that they cannot take antibiotics or that they must be taken with extreme caution and strictness.
Thus, individual intolerance to a particular drug will be the first reason for refusing a particular antibiotic.
The second reason may be the child's allergies. If your baby is prone to such reactions, you should think about prescribing antibiotics again.
Intestinal dysbiosis is another contraindication to taking antibiotics. Serious microflora disturbances combined with the use of strong drugs can literally “kill” the natural immunity of a very young organism.
Infectious mononucleosis, severe liver disease and lymphocytic leukemia are not a complete list of diagnoses that are a beacon prohibiting the use of certain antibiotics.
This is not a complete list of contraindications for children under one year old. Remember that each case should be discussed individually with your doctor.
“At 11.5 months, my son was prescribed an antibiotic, but a very gentle one. I would not have resorted to it if it were not for the unsuccessful treatment for three weeks. We took it for only 3 days - that’s exactly what the doctor prescribed. During the appointment, a slight diarrhea began, which was dealt with with Smecta.”
Happy mother Katerina Kharitonova
What should we not forget?
Why shouldn’t you take an antibiotic off the shelf immediately after the first signs of illness?
There are a number of arguments that will help parents understand that antibiotics for a child under one year of age are a serious step and a responsibility for their health. Firstly, as we mentioned above, antibiotics can pose a threat to the immunity of a very tiny and not yet strong organism. In the first months of life, protection from adverse external influences (viruses and infections) is formed at a rapid pace, but it is during this period that you need to be especially careful about children's health.
Careless administration of potent substances can destroy or slow down the natural development processes of your baby’s body’s defense system. Think about this if, contrary to our advice, you decide to run for an antibiotic at the slightest increase in temperature.
Secondly, do not forget about the side effects of antibiotics. At the slightest deviation from the instructions and the individual characteristics of the child’s body, the reaction to the drug can be very unpleasant. Side effects of most antibiotics include:
- digestive disorders (digestive system disorders, prolonged dysbacteriosis;
- allergic reactions;
- damage to liver and kidney tissues;
- neurotoxic effect;
- hematological disorders;
- dermatitis;
- avitaminosis.
Thirdly, it is necessary to be very strict about the doctor’s recommendations on the dosage of the drug. A child under one year old is too small to absorb a whole dose, so most often parents have to adapt to the specific age (month) and weight of the child. This is very important, since if the antibiotic dosage is not observed, treatment can be either useless or dangerous for the baby.
Fourthly, for the same reason, it is important not to interrupt antibiotic treatment without permission and to complete what you started. Very often, at the first sign of relief, parents stop giving the antibiotic (although your doctor will likely tell you that this is important), and the symptoms either return or lead to new ones. Is it worth saying again that antibiotics are not a toy?
Taking antibiotics in infants: indications and consequences
Antibiotics are an effective means of combating pathogenic bacteria. But despite such valuable quality of these drugs, their use is fraught with the development of many adverse consequences. Details about what an antibiotic is for a baby, when it is needed, how to give it to a baby correctly and what consequences to expect can be found in this article.
What antibiotics can infants take?
The very first and most important answer to this question will be - only those prescribed by the pediatrician. Antibacterial drugs should not be used as a means of self-medication in infancy.
All antibiotics are divided into:
- to those that completely destroy the pathogenic microbe (bactericidal);
- and those that prevent and make their further reproduction impossible (bacteriostatic).
Some drugs have a narrow spectrum of action and fight a specific microbe; in most cases, they do not have a significant effect on the child’s microflora. Others have a wide range of effects and affect all human microorganisms. As a result of their use, dysbacteriosis and thrush occur.
The property of some antibacterial drugs to accumulate at the site of bacterial inflammation is considered important. For example:
- Ampicillin in otitis media accumulates in the middle ear;
- Polymyxin acts only in the intestinal lumen;
- Azithromycin always targets the infectious focus.
Penicillins, Amoxicillins, Ceftriaxone and Azithromycin are often used in pediatric practice. Depending on the nature of the pathogen and the development of the disease, the appointment and administration of antibiotics is an individual process.
When do children under one year old need antibiotics?
Taking drugs from this group is justified only if the infant has a bacterial infection, both primary and as a result of the development of complications during ARVI.
Unfortunately, the prescription of these drugs for acute respiratory viral infections for the purpose of prevention is widespread and encouraged by both mothers and doctors. This approach is fundamentally incorrect and can not only cause adverse reactions, but also significantly increase the likelihood of complications.
Signs of the development of bacterial complications in ARVI:
- There is no tendency to improve the condition on the 4th day of illness;
- Maintaining a high body temperature for 7 days;
- Temporary improvement followed by worsening of the condition;
- With minor catarrhal manifestations, the severity of the condition is pronounced;
- A combination of symptoms such as: pallor, thirst, very intense pain, difficulty breathing, discharge of pus from any location (nose, eyes, ears);
- Increased cough;
- Ineffectiveness of antipyretic drugs.
In the presence of such clinical phenomena, it is possible to suspect the probable course of a bacterial process. But only a doctor should confirm this and make a decision about prescribing an antibiotic for the baby.
For example, treatment of bronchitis in infants with antibiotics begins only after confirmation of the diagnosis by X-ray examination. It is important that if complications develop, a child under one year of age should not be treated at home.
How to give an antibiotic to a baby
If for some reason antibiotic treatment is carried out at home, it is important to strictly follow the doctor's instructions. How many days an antibiotic is given to infants will depend on the nature of the disease and the dynamics of symptoms. On average, the course takes 5 days.
When taking an antibacterial drug, the following conditions must be met:
- The dose of medication is calculated individually for each child, based on his age and body weight;
- While taking an antibiotic, the child should not go hungry;
- Mandatory compliance with the drinking regime;
- Give the baby the drug strictly at certain intervals with the established frequency of administration;
- Independently increasing or decreasing the dose is unacceptable;
- Even with a significant improvement in the condition, you cannot stop taking the drug;
- The minimum duration of antibiotic treatment is 3 days;
- The medicine is given by mouth in the form of suspensions;
- The required amount of the drug is determined by a special measuring spoon or syringe.
Along with the treatment with an antibacterial drug, it is important to follow the recommendations for the baby’s nutrition and create optimal microclimate conditions - all this prevents the mucus from drying out and speeds up the healing process.
Consequences of taking antibacterial drugs
If antibiotics are thoughtlessly prescribed to an infant, the consequences will not be long in coming. The most common allergy to antibiotics occurs in infants, which can manifest itself in a variety of forms from rashes to Quincke's edema and anaphylactic shock.
The baby's microflora suffers after broad-spectrum antibiotics. As a result of treatment, not only harmful bacteria are killed, but also beneficial intestinal flora. As a result, an imbalance occurs among representatives of the microbiota, which is manifested by signs of disruption of the gastrointestinal tract.
In addition, some drugs have a toxic effect on the baby’s body, which is expressed in the manifestation of:
- Nephrotoxicity – damage to the kidney tubules;
- Neurotoxicity - a pathological effect on nervous tissue, especially dangerous for children who already have any pathology of the nervous system;
- Ototoxicity – damage to the auditory nerve, which can lead to complete hearing loss;
- Hepatotoxicity – damage to liver cells.
Antibiotics are drugs that can have not only positive effects, but also many adverse effects.
The dangers of self-medication with antibiotics
Self-prescription and use of antibacterial drugs is fraught with the development of conditions such as:
- Worsening and prolongation of the course of the disease due to improper selection of an antibacterial agent;
- Development of severe allergic reactions;
- If not treated or the wrong dosage is used, some of the bacteria remain and form a stable form;
- Side effects from the use of the drug can aggravate the course of the underlying disease;
- The consequences after taking an antibiotic are sometimes more severe;
- Use for ARVI increases the likelihood of bacterial complications.
The use of antibacterial agents for bacterial infections is logical and mandatory. But prescribing such serious medications to an infant should be carefully considered. It is necessary to take into account many different factors in order to maximally protect the baby from adverse consequences. Therefore, only a doctor prescribes antibacterial drugs.
Valentina Ignasheva, pediatrician, especially for Mirmam.pro
Source: //mirmam.pro/antibiotiki-grudnichkam
Indications for the use of antibiotics in infants
Many parents do the wrong thing when they try to treat a cold with antibiotics. This disease is caused by viruses. Only antiviral drugs are effective against them. Antibiotics are prescribed to children under one year of age only when the disease is caused by bacteria. Characteristic signs of a bacterial cold:
- purulent plaque on the laryngeal mucosa;
- sore throat;
- temperature rise in the first couple of days to high levels;
- nausea;
- headache;
- diarrhea.
Antibiotics for children under 1 year of age are also prescribed for other types of bacterial infections. The main indications for their use in childhood:
- otitis;
- sinusitis;
- meningitis;
- pneumonia;
- pyelonephritis;
- purulent sore throat;
- scarlet fever;
- cystitis;
- paratonsillitis;
- dysentery;
- cholera.

Use of antibacterial drugs in children
The physiological characteristics of the child’s body, leading to changes in the pharmacokinetics of drugs, can have a significant impact on the choice and dosage of anti-infective chemotherapy drugs. The use of some of them in pediatrics is prohibited or limited due to the risk of severe, often age-specific, adverse reactions.The use of AMPs in newborns, especially premature infants, requires the greatest attention, which is due to the immaturity of the enzymatic systems of the liver and the mechanisms of glomerular filtration of the kidneys, as well as changes in the distribution of drugs due to the larger volume of extracellular fluid in newborns. When prescribing AMPs that have a high affinity for plasma proteins (sulfonamides, ceftriaxone), lower serum albumin concentrations in newborns and the associated risk of kernicterus are important. Wrong choice of drug or its dose, lack of monitoring of antibiotic concentrations in the blood can lead to severe complications of antibiotic therapy (for example, “gray syndrome” when using chloramphenicol). Given the importance of this problem, the dosage of antibacterial agents in newborns is included in a separate table.
Below are the features of the use of individual AMPs in pediatrics. Warnings regarding the prescription of other drugs to children are indicated when describing the pharmacological characteristics of these drugs.
Aminoglycosides
- the volume of distribution in the body of newborns is larger than that of adults, therefore the dose of drugs per kilogram of body weight in newborns is higher. The half-life is increased due to a decrease in the glomerular filtration rate, which requires correction of the intervals between administrations.
Chloramphenicol
- inactivation of the drug is slowed down due to the immaturity of liver enzymes in newborns, high concentrations are created in the blood plasma. In order to prevent the “gray syndrome” and severe hematopoietic lesions, monitoring of blood concentrations and hematological parameters is necessary. Chloramphenicol should not be given to newborns unless a safer alternative is available.
Sulfonamides and co-trimoxazole
- increased risk of kernicterus, due to the competitive displacement of bilirubin from binding with plasma proteins, and hemolytic anemia caused by deficiency of glucose-6-phosphate dehydrogenase. Contraindicated in newborns, with the exception of the treatment of congenital toxoplasmosis and Pneumocystis pneumonia.
Ceftriaxone
- increased risk of kernicterus in newborns and complications from the gastrointestinal tract in childhood. Prescribing the drug to newborns should be avoided; if necessary, use cefotaxime. It should be prescribed with caution in high doses to children with diseases of the gallbladder and pancreas.
Penicillins, cephalosporins, carbapenems, monobactams
- the half-life from the body is increased due to a reduced glomerular filtration rate and tubular secretion. Dosage adjustments or intervals between administrations may be required.
Tetracyclines
- risk of undesirable effects on bone tissue and teeth. Contraindicated in children under 8 years of age (unless a safer alternative is not available).
Nitrofurans
- risk of hemolytic anemia due to glucose-6-phosphate dehydrogenase deficiency. Contraindicated for newborns.
Quinolones/fluoroquinolones
- the risk of impaired formation of the osteoarticular system (based on experimental data) and hemolytic anemia with deficiency of glucose-6-phosphate dehydrogenase. The use of quinolones in children under 3 years of age is undesirable. Fluoroquinolones are not officially approved for use in children, but according to international experts they can be prescribed for severe infections when there is no alternative.
Table 1. Average daily doses of antibacterial agents in children aged 1 month to 12 years*
| 3 | ||
| Antibacterial drugs | ||
| Penicillins | ||
| Azlocillin | 200-300 mg/kg/day in 4 administrations; IV | |
| Amoxicillin | 30-60 mg/kg/day in 3 divided doses | |
| Amoxicillin/clavulanate | 40-60 mg/kg/day in 3 divided doses2 | 40-60 mg/kg/day** in 3 administrations; IV |
| Ampicillin | 30-50 mg/kg/day in 4 divided doses | 50-100 mg/kg/day in 4 administrations; i/m, i/v |
| Ampicillin/sulbactam | 50 mg/kg/day in 2 divided doses | 150 mg/kg/day in 3-4 administrations; i/m |
| Benzylpenicillin | 50-150 IU/kg/day in 4 administrations; i/m, i/v | |
| Benzylpenicillin procaine | 50-100 thousand units/kg/day in 1-2 administrations; i/m | |
| Benzathine benzylpenicillin | 50 thousand units/kg/day in 1-2 administrations; i/m | |
| Benzylpenicillin (potassium salt)/ Benzylpenicillin procaine/ Benzathine benzylpenicillin (1:1:1) ( Bicillin-3 ) | Dosed according to benzathine benzylpenicillin | |
| Benzylpenicillin/benzathine benzylpenicillin (4:1) ( Bicillin-5 ) | Dosed according to benzathine benzylpenicillin | |
| Carbenicillin | 400-600 mg/kg/day in 6-8 administrations; i/m, i/v | |
| Oxacillin | 40-60 mg/kg/day (but not more than 1.5 g/day) in 3-4 doses | 200-300 mg/kg/day in 4-6 injections; i/m, i/v |
| Piperacillin | 150-300 mg/kg/day in 3-4 administrations; IV | |
| Ticarcillin/clavulanate | 200-300 mg/kg/day*** in 4-6 injections; IV | |
| Phenoxymethylpenicillin | 30-40 mg/kg/day in 4 divided doses | |
| Cephalosporins | ||
| Cefazolin | 50-100 mg/kg/day in 2-3 administrations; i/m, i/v | |
| Cefaclor | 20-40 mg/kg/day in 2-3 doses | |
| Cephalexin | 45 mg/kg/day in 3 divided doses | |
| Cefepime | > 2 months - 50 mg/kg/day in 3 doses; IV | |
| Cefixime | > 6 months - 8 mg/kg/day in 1-2 doses | |
| Cefoperazone/sulbactam | 40-80 mg/kg/day in 2-3 administrations; i/m, i/v | |
| Cefoperazone | 50-100 mg/kg/day 2-3 administrations; i/m, i/v | |
| Cefotaxime | 50-100 mg/kg/day in 2-3 administrations; i/m, i/v | |
| Ceftazidime | 30-100 mg/kg/day in 2-3 administrations; i/m, i/v | |
| Ceftibuten | 1-10 years - 9 mg/kg/day in 1-2 doses 10-12 years (body weight > 45 kg) - 200-400 mg/day in 1-2 doses | |
| Ceftriaxone | 20-75 mg/kg/day in 1-2 administrations; i/m, i/v | |
| Cefuroxime | 50-100 mg/kg/day in 3-4 administrations; i/m, i/v | |
| Cefuroxime-axetil | 30-40 mg/kg/day in 2 divided doses with meals | |
| Carbapenems | ||
| Imipenem | 60-100 mg/kg/day (up to 2 g/day) in 3-4 administrations; IV | |
| Meropenem | > 3 months - 60 mg/kg/day in 3-4 administrations; IV | |
| Monobactams | ||
| Aztreons | 120-150 mg/kg/day in 3-4 administrations; IV | |
| Aminoglycosides | ||
| Amikacin | 15-20 mg/kg/day in 1-2 administrations; i/m, i/v | |
| Gentamicin | 3-5 mg/kg/day in 1-2 administrations; i/m, i/v | |
| Netilmicin | 4-7.5 mg/kg/day in 1-2 administrations; i/m, i/v | |
| Streptomycin | 15-20 mg/kg/day (no more than 2 g/day) per 1 administration; i/m | |
| Tobramycin | 3-5 mg/kg/day in 1-2 administrations; i/m, i/v | |
| Macrolides | ||
| Azithromycin | 3-day course : 10 mg/kg/day or 5-day chicken with: 10 mg/kg on the 1st day, then 5 mg/kg/day | |
| Josamycin | 30-50 mg/kg/day | |
| Clarithromycin | > 6 months - 15 mg/kg/day in 2 divided doses | |
| Midecamycin | 30-50 mg/kg/day in 2-3 doses | |
| Roxithromycin | 5-8 mg/kg/day in 2 divided doses | |
| Spiramycin | 150 thousand IU/kg/day in 2 divided doses | |
| Erythromycin | 40-50 mg/kg/day in 3-4 doses | 40-50 mg/kg/day in 3-4 administrations; IV |
| Tetracyclines | ||
| Doxycycline | > 8 years - 5 mg/kg/day (but not more than 200 mg/day) in 1-2 doses | > 8 years - on the 1st day 5 mg/kg, then 2.5 mg/kg/day in 2 administrations; IV |
| Tetracycline | > 8 years - 25-50 mg/kg/day (but not more than 3 g/day) in 4 doses | |
| Quinolones/Fluoroquinolones | ||
| Nalidixic acid | > 3 months - 55 mg/kg/day in 4 doses | |
| Oxolinic acid | > 2 years - 500 mg/day in 2 doses | |
| Pipemidic acid | > 1 year - 15 mg/kg/day in 2 divided doses | |
| Ciproflocacin4 | For health reasons, children - 10-15 mg/kg/day in 2 divided doses (but not more than 1.5 g/day) | For health reasons - 7.5-10 mg/kg/day (but not more than 800 mg/day) in 2 administrations; IV |
| Glycopeptides | ||
| Vancomycin | 40-60 mg/kg/day (but not more than 2 g/day) in 4 administrations; IV | |
| Teicoplanin | 6-10 mg/kg/day in 2 administrations; i.v., i.m. | |
| Oxazolidinones | ||
| Linezolid | і 5 years : 10 mg/kg (but not more than 0.6 g) every 12 hours | і 5 years : 10 mg/kg (but not more than 0.6 g) every 12 hours. |
| Lincosamides | ||
| Clindamycin | 10-25 mg/kg/day (but not more than 2 g/day) in 3-4 doses | 20-40 mg/kg/day (but not more than 3g/day) in 3-4 administrations; i/m, i/v |
| Lincomycin | 30-60 mg/kg/day in 3-4 doses | 10-20 mg/kg/day in 2 administrations; i/m, i/v |
| Nitroimidazoles | ||
| Metronidazole | 22.5 mg/kg/day in 3 divided doses | 22.5 mg/kg/day in 3 administrations; IV |
| Ornidazole | 25-40 mg/kg/day in 1-2 doses | |
| Tinidazole | 50-60 mg/kg/day in 1 dose | |
| Nitrofurans | ||
| Nitrofurantoin | 5-7 mg/kg/day in 4 divided doses | |
| Nifuratel | 10-20 mg/kg/day in 2-3 doses | |
| Nifuroxazide | 1 month-2.5 years - 0.1 g every 8-12 hours; > 2.5 years - 0.2 g every 8 hours | |
| Furazolidone | 6-7 mg/kg/day in 4 divided doses | |
| Furazidin | 7.5 mg/kg/day in 2-3 doses | |
| Polymyxins | ||
| Polymyxin B | 1.5-2.5 mg/kg/day (but not more than 200 mg/day) in 3-4 administrations; i/m, i/v | |
| Polymyxin M | < 5 years - 100 thousand units/kg/day in 3 divided doses 5-12 years - 1.5 million units/day in 3-4 divided doses | |
| Sulfonamides and co-trimoxazole | ||
| Sulfadiazine | > 2 months - 75 mg/kg for the first dose, then 37.5 mg/kg every 6 hours or 25 mg/kg every 4 hours (but not more than 6.0 g/day) | |
| Sulfadimidine | > 2 months - 100 mg/kg for the first dose, then 25 mg/kg every 4-6 hours | |
| Co-trimoxazole | > 2 months - 6-8 mg/day**** in 2 divided doses | > 2 months - for severe infections, including Pneumocystis pneumonia, 15-20 mg/kg/day**** in 3-4 administrations |
| Drugs of other groups | ||
| Nitroxoline | 5-8 mg/kg/day in 2-3 doses | |
| Spectinomycin | Body weight < 45 kg - 40 mg/kg once; Body weight > 45 kg - 2 g once; i/m | |
| Fosfomycin | > 5 years - 2 g/day in 1 dose | |
| Fusidic acid | < 1 year - 50 mg/kg/day in 3 divided doses 2-5 years - 0.75 g/day in 3 divided doses 6-12 years - 1.5 g/day in 3 divided doses | 20 mg/kg/day in 3 administrations; IV |
| Chloramphenicol | < 1 year - 50-75 mg/kg/day in 4 divided doses | 50-75 mg/kg/day in 4 administrations; i/m, i/v |
| Anti-tuberculosis drugs | ||
| Isoniazid | 10-15 mg/kg/day (but not more than 0.3 g/day) in 1-2 doses | 10-15 mg/kg/day (but not more than 0.3 g/day) in 1-2 administrations; i/m |
| Capreomycin | 15-30 mg/kg/day (but not more than 1 g/day) per 1 administration; i/m | |
| Metazide | 20-30 mg/kg/day in 2-3 doses | |
| PASK | 200-300 mg/kg/day (but not more than 12 g/day) in 2-3 doses | |
| Pyrazinamide | 20-40 mg i/kg/day in 1 dose | |
| Prothionamide | 15-20 mg/kg/day (but not more than 1 g/day) in 1-3 doses | |
| Rifampicin | 10-20 mg/kg/day (but not more than 0.6 g/day) in 1 dose | |
| Streptomycin | 20 mg/kg/day in 1 administration; i/m | |
| Thioacetazone | 4 mg/kg/day in 1 dose | |
| Cycloserine | 10-20 mg/kg/day (but not more than 1 g/day) in 2 divided doses | |
| Ethambutol | 15-25 mg/kg/day (but not more than 2.5 g/day) in 1 dose | |
| Ethionamide | 15-20 mg/kg/day (but not more than 1 g/day) in 1-3 doses | |
| Antifungal drugs | ||
| Amphotericin B | Test dose 1 mg in 20 ml of 5% glucose for 1 hour; i.v. Therapeutic dose is 0.3-1.5 mg/kg/day in 1 administration; IV | |
| Amphotericin B liposomal | 1-5 mg/kg/day in 1 administration; IV | |
| Griseofulvin | 10 mg/kg/day in 1-2 doses | |
| Potassium iodide | Beginning dose - 5 drops. every 8-12 hours, then once. the dose is increased by 5 drops/week and adjusted to 25-40 drops. every 8-12 hours | |
| Ketoconazole | 3 mg/kg/day | |
| Levorin | < 6 years - 20-25 thousand units/kg every 8-12 hours; > 6 years - 250 thousand units every 8-12 hours | |
| Natamycin | 0.1 g every 12 hours | |
| Nystatin | 125-250 thousand units every 6 hours | |
| Terbinafine | > 2 years : body weight < 20 kg - 62.5 mg/day, 20-40 kg - 0.125 g/day, > 40 kg - 0.25 g/day, in 1 dose | |
| Fluconazole | For candidiasis of the skin and mucous membranes - 1-2 mg/kg/day in 1 dose; for systemic candidiasis and cryptococcosis - 6-12 mg/kg/day in 1 dose | For candidiasis of the skin and mucous membranes - 1-2 mg/kg/day in 1 administration; i.v.; for systemic candidiasis and cryptococcosis - 6-12 mg/kg/day in 1 administration; IV |
| Antiviral drugs | ||
| Antiherpetic drugs | ||
| Acyclovir | In children <12 years of age, the dose is calculated per body surface area: 0.25 g/m2 instead of 5 mg/kg, 0.5 g/m2 instead of 10 mg/kg For chickenpox in children under 2 years of age, 80 mg/kg/day 4 doses, 2-16 years - 20 mg/kg (but not more than 0.8 g) every 6 hours | 5 mg/kg every 8 hours; IV |
| Anticytomegaloviral drugs | ||
| Ganciclovir | 5 mg/kg every 12 hours, IV | |
| Foscarnet | 90 mg/kg every 12 hours, or 60 mg/kg every 8 hours; IV | |
| Anti-flu drugs | ||
| Amantadine | > 1 year : 5 mg/kg/day (but not more than 0.15 g) in 2 divided doses | |
| Arbidol | 2-6 years : for treatment - 0.05 g every 6 hours 6-12 years: for treatment - 0.1 g every 6 hours; for prevention - 0.1 g/day | |
| Zanamivir | > 7 years : 0.01 g every 12 hours | |
| Rimantadine | > 1 year : 5 mg/kg/day (but not more than 0.15 g) in 2 divided doses | |
| Extended spectrum antivirals | ||
| Interferon alpha | > 1 year : 3-6 million IU/m2 body surface 3 times a week; s/c or i/m | |
| Lamivudine | for CHB (in children > 2 years old) - 3 mg/kg/day (but not more than 0.1 g); for HIV infection - < 1 month - 2 mg/kg every 12 hours, 1 month-12 years - 4 mg/kg every 12 hours (but not more than 0.3 g/day) | |
| Ribavirin | Inhalation (via nebulizer) For RSV infection - 20 mg/ml/day (6.0 g in 300 ml of sterile water) for 18 hours | |
| Antiretroviral drugs | ||
| Abacavir | > 3 months : 8 mg/kg every 12 hours (but not more than 0.6 g/day) | |
| Amprenavir | > 4 years : caps. - 20 mg/kg every 12 hours or 15 mg/kg every 8 hours; solution - 22.5 mg/kg every 12 hours or 17 mg/kg every 8 hours | |
| Didanosine | Body surface 2 - 0.025 g (tablets) and 0.031 g (powder), 0.5-0.7 m2 - 0.05 g and 0.062 g (respectively), 0.8-1.0 m2 - 0.075 g and 0.094 g (resp.), 1.1-1.4 m2 - 0.1 g and 0.125 g (resp.); every 12 hours | |
| Zidovudine | > 3 months : 60 mg/m2 every 8 hours (480 mg/m2 per day) | |
| Ifavirenz | > 3 years: body weight 13-15 kg - 0.2 g/day, 15-20 kg - 0.25 g/day, 20-25 kg - 0.3 g/day, 25-32 kg - 0.35 g/day, 32-40 kg - 0.4 g/day | |
| Nevirapine | 2 months-8 years - 4 mg/kg/day in 1 dose for 2 weeks, then 7 mg/kg every 12 hours; > 8 years - 4 mg/kg/day in 1 dose for 2 weeks, then 4 mg/kg every 12 hours Maximum daily dose - 0.4 g | |
| Nelfinavir | > 2 years : 20-30 mg/kg every 8 hours | |
| Ritonavir | > 2 years : 0.4 g/m2 every 12 hours. If poorly tolerated - 0.25 g/m2, followed by increasing the dose every 2-3 days by 50 mg/m2 until the standard dose is reached | |
| Stavudin | < 30 kg : 1 mg/kg every 12 hours > 30 kg : 0.015 g every 12 hours | |
| Antiprotozoal drugs | ||
| Artemether | 1st dose - 3.2 mg/kg, then 1.6 mg/kg/day; i/m | |
| Artesunate | on the 1st day - 2 mg/kg every 12 hours, then - 1 mg/kg every 12 hours; IV | |
| Halofantrine | > 1 year : 8 mg/kg - in 3 doses every 6 hours | |
| Dehydroemetine | 1 mg/kg/day (not more than 0.09 g); i/m | |
| Diloxanide furoate | > 2 years : 20 mg/kg/day in 3 divided doses | |
| Meglumine antimonate | 20 mg antimony/kg/day; i/m | |
| Mefloquine | > 2 years : for the treatment of malaria - 15 mg/kg once; for prevention - 5 mg/kg/week | |
| Paromomycin | 25-30 mg/kg/day in 3 divided doses | |
| Pyrimethamine | Treatment of toxoplasmosis for the first 2 days - 2 mg/kg/day, then 1 mg/kg/day | |
| Pyrimethamine/sulfadoxine | J 4 years - 1/2 tablet, 5-8 years - 1 tablet, > 9 years - 2 tablets, once | Up to 1 year - 1/4 amp., 1-4 years - 1/4-3/4 amp., 5-8 years - 3/4-1 amp., > 9 years - 1-1.5 amp, once ; i/m |
| Primaquin | > 3 years : 0.25 mg/kg/day or 0.75 mg/kg/week Calculation on primaquine base | |
| Proguanil | 3 mg/kg/day | |
| Quinine | 25 mg/kg/day in 3 doses every 8 hours. Calculation on quinine base | 25 mg/kg/day in 3 injections every 8 hours. Calculation on quinine base. |
| Chloroquine | Treatment of malaria 1st dose - 10 mg/kg, after 6 hours 2nd dose - 5 mg/kg, on the 2nd and 3rd days - 5 mg/kg Prevention of malaria 5 mg/kg/week Calculation on chloroquine base | Treatment of malaria 1st dose - 10 mg/kg, after 6 hours 2nd dose - 5 mg/kg, on the 2nd and 3rd days - 5 mg/kg (if possible avoid IV administration ) Calculation for chloroquine base. |
| Emetine | 1 mg/kg/day (not more than 0.06 g); i/m | |
| Etofamide | 20 mg/kg/day in 2 divided doses | |
| Anthelmintic drugs | ||
| Diethylcarbamazine | > 6 years : 6 mg/kg/day in 3 divided doses | |
| Ivermectin | > 5 years : for helminthiases - 0.15-0.2 mg/kg once; for scabies - 0.2 mg/kg once | |
| Levamisole | For ascariasis, 2.5 mg/kg once; for enterobiasis - two doses of 2.5 mg/kg with an interval of 7-10 days | |
| Mebendazole | > 2 years : for ascariasis and enterobiasis - 0.2-0.4 g once; for hookworm - 0.4 g/day, 3 days; for strongyloidiasis - 0.4-0.8 g every 12-24 hours, 3-5 days; for trichocephalosis - 0.4 g/day, 1-3 days; for trichinosis - 10 mg/kg/day in 3 doses, 7-10 days; for toxocariasis - 10 mg/kg/day in 3 doses, 10-20 days, for echinococcosis - 10-20 mg/kg/day in 2-3 doses, several months | |
| Niclosamide | &dt; 2 years - 0.5 g; 2-5 years - 1.0 g; 6-12 years - 1.5 g, once | |
| Pyrantela pamoate | &dt; 2 years - once. dose 62.5 mg; 2-6 years - 0.125 g; 6-12 years - 0.25 g; 12-15 years - 0.375 g. For ascariasis - once; for hookworm - 3 days, for enterobiasis - 2 doses with an interval of 7-10 days | |
| Praziquantel | > 4 years : for opisthorchiasis, clonorchiasis and paragonimiasis - 75 mg/kg/day in 3 doses, 1 day; for schistosomiasis - 40-75 mg/kg/day in 2-3 doses, 1 day; for hymenolepidosis - 2 doses of 20-25 mg/kg with an interval of 10 days; for other cestodes - 20-25 mg/kg once | |
- When treating some infections, doses may be higher or lower than indicated; doses for children over 12 years of age correspond to doses for adults - For amoxicillin *** - For ticarcillin **** - For trimethoprim
Table 2. Average doses of antibacterial drugs in newborns*
| A drug | Route of administration | Single doses (mg/kg)/intervals between administrations | ||||
| Body weight < 1.2 kg | Body weight 1.2-2 kg | Body weight > 2 kg | ||||
| 0-4 days | 0-7 days | > 7 days | 0-7 days | > 7 days | ||
| 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| Penicillins | ||||||
| Ampicillin | IV, IM | 25/12 h | 25/12 h | 25/6-8 h | 25/8 h | 25/6 h |
| Benzylpenicillin | IV | 25 thousand units/12 hours | 25 thousand units/12 hours | 25 thousand units/8 hours | 25 thousand units/8 hours | 25 thousand units 6 hours |
| Benzylpenicillin procaine | V/m | 50 thousand units/24 hours | 50 thousand units/24 hours | 50 thousand units/24 hours | 50 thousand units/24 hours | 50 thousand units/24 hours |
| Oxacillin | IV, IM | 25/12 h | 25/12 h | 30/8 h | 25/8 h | 37.5/6 h |
| Cephalosporins | ||||||
| Cefazolin | IV, IM | 20/12 h | 20/12 h | 20/12 h | 20/12 h | 20/8 h |
| Cefotaxime | IV, IM | 50/12 h | 50/12 h | 50/8 h | 50/12 h | 50/8 h |
| Ceftazidime | IV, IM | 30-50/12 h | 30-50/8 h | 30-50/8 h | 30-50/8 h | 30-50/8 h |
| Ceftriaxone | IV, IM | 50/24 h | 50/24 h | 50/24 h | 50/24 h | 50/24 h |
| Carbapenems | ||||||
| Imipenem | IV, IM | 25/18-24 h | 25/12 h | 25/12 h | 25/12 h | 25/8 h |
| Monobactams | ||||||
| Aztreons | IV, IM | 30/12 h | 30/12 h | 30/8 h | 30/8 h | 30/6 h |
| Aminoglycosides | ||||||
| Amikacin | IV, IM | 7.5/18-24 hours | 7.5/12-18 h | 7.5/8-12 h | 10/12 h | 10/8 h |
| Gentamicin | IV, IM | 2.5/18-24 hours | 2.5/12-18 hours | 2.5/12-18 hours | 2.5/12 h | 2.5/8 h |
| Netilmicin | IV, IM | 2.5/18-24 hours | 2.5/12 h | 2.5/8 h | 2.5/12 h | 2.5/8 h |
| Streptomycin | V/m | 10-15/12 h | 10-15/12 h | 10-15/12 h | 10-15/12 h | 10-15/12 h |
| Tobramycin | IV, IM | 2-2.5/12 h | 2-2.5/12 h | 2-2.5/8 h | 2-2.5/12 h | 2-2.5/8 h |
| Macrolides | ||||||
| Erythromycin | Inside | 10/12 h | 10/12 h | 10/8 h | 10/12 h | 10/8 h |
| Glycopeptides | ||||||
| Vancomycin | IV | 15/18-36 h | 15/12-18 h | 15/8-12 h | 15/12 h | 15/8 h |
| Lincosamides | ||||||
| Clindamycin | IV, IM, inside | 5/12 h | 5/12 h | 5/8 h | 5/8 h | 5/6 h |
| Nitroimidazoles | ||||||
| Metronidazole | IV, inside | 7.5/48 h | 7.5/24 h | 7.5/12 h | 7.5/12 h | 15/12 h |
| Drugs of other groups | ||||||
| Co-trimoxazole** | IV, inside | 5/48 h | 5/48 h | 5/24 h | 5/48 h | 5/24 h |
| Chloramphenicol | IV, IM, inside | 25/24 h | 25/24 h | 25/24 h | 25/24 h | 25/12 h |
| Anti-tuberculosis drugs | ||||||
| Isoniazid | Inside | 5/24 h | 5/24 h | 5/24 h | 5/24 h | 5/24 h |
| Pyrazinamide | Inside | 35/24 h | 35/24 h | 35/24 h | 35/24 h | 35/24 h |
| Antifungal drugs | ||||||
| Amphotericin B | IV | 0.25/24 h | 0.25/24 h | 0.25/24 h | 0.25/24 h | 0.25/24 h |
| Amphotericin B liposomal | IV | 1-3/24 h | 1-3/24 h | 1-3/24 h | 1-3/24 h | 1-3/24 h |
| Antiviral drugs | ||||||
| Acyclovir | IV | 10/8 h | 10/8 h | 10/8 h | 10/8 h | 10/8 h |
| Ganciclovir*** | IV | 5/12 h | 5/12 h | 5/12 h | 5/12 h | 5/12 h |
| Interferon alpha | PC | 3 million units/m2/3 times per week | 3 million units/m2/3 times per week | 3 million units/m2/3 times per week | 3 million units/m2/3 times per week | 3 million units/m2/3 times per week |
| Ribavirin | Ing.**** | 20/24 h | 20/24 h | 20/24 h | 20/24 h | 20/24 h |
| Antiparasitic drugs | ||||||
| Proguanil | Inside | 3/24 h | 3/24 h | 3/24 h | 3/24 h | 3/24 h |
| Quinine | Inside | 10/8 h | 10/8 h | 10/8 h | 10/8 h | 10/8 h |
— Doses for the treatment of meningitis are given in the section “CNS infections” — For trimethoprim *** — In case of very low body weight and renal failure, the intervals between doses should be increased **** — Inhalation via nebulizer
Types of antibiotics for children
Common forms of antibiotics are tablets, capsules, granules and injection solutions. They also exist in the form of drops, which are used for inhalation and rinsing. Local treatment is carried out using sprays. The most popular among them is Bioparox. Syrups are used for children under 10 years of age. This release form has a pleasant smell and taste.
For babies under 1 year of age, pediatric antibiotics in suspension are more convenient, since at this age they do not yet have the ability to swallow tablets. Depending on the active component, drugs are divided into several groups. General scheme for preparing a suspension from dry matter:
- Using a special syringe for measurements (usually it comes with an antibiotic), draw 12 ml of boiled water or another amount specified in the instructions.
- Add it to the bottle to the powder up to the mark or pour in the crushed tablet, shake the contents well so that there are no lumps.
- Keep in the refrigerator between doses. Store for no more than 5 days.
Penicillin antibiotics for children
Drugs from the penicillin category have broad antibacterial activity. In most cases, they are the first antibiotics prescribed. Penicillins have low toxicity. This group contains the largest number of safe drugs that are approved from birth.
Penicillins disrupt bacterial cell wall synthesis, but microorganisms can quickly develop resistance to these drugs. Diseases for which these antibiotics are used:
- scarlet fever;
- skin infections;
- tonsillitis;
- otitis;
- acute sinusitis;
- streptococcal sepsis;
- pneumonia;
- septic-toxic diphtheria;
- purulent meningitis;
- umbilical sepsis.
Amoxicillin
Amoxicillin suspension is used to treat children under 5 years of age. It is prepared immediately before use. One measuring spoon contains 5 milliliters of suspension and 250 milligrams of amoxicillin. Dosage for children under 2 years of age – no more than 20 mg/kg/day. Amoxicillin is used alone or in combination with clavulanic acid. Indications for antibiotic use:
- shigellosis;
- meningitis;
- endocarditis;
- borreliosis;
- salmonellosis;
- sepsis;
- leptospirosis;
- cystitis;
- urethritis;
- gonorrhea;
- bronchitis;
- angina;
- pneumonia;
- pyelonephritis.
Augmentin
Treatment with Augmentin is prescribed not only for infections caused by microorganisms sensitive to this antibiotic. The drug is also used in cases of diseases caused by bacteria that are affected by amoxicillin. The scope of Augmentin is extensive. The list of indications includes:
Diseases of the ENT organs and respiratory tract
Urogenital tract infections
Newborns and children from 3 months to 12 years old with a body weight of up to 40 kg are prescribed a suspension of 125/31.25 mg in a dose of 5 ml 3 times a day. every 8 hours, and the drug 200/28.5 or 400/57 milligrams - 2 times/day. after 12 hours. The daily dose for infants under this age is 30 mg/kg, divided into 2 doses. Augmentin is prescribed in high or low dosages depending on the disease. Doctors recommend the following regimens:
Suspension 4:1, frequency of administration – 3 times/day. (mg/kg/day)
Suspension 7:1, frequency of administration – 2 times/day. (mg/kg/day)
When should a baby be given antibiotics?
Antibiotics are medications that have the ability to destroy bacteria or suppress their reproduction. Many parents are wary of prescribing them to their children because of the risk of side effects.
What diseases require the use of antibacterial agents? Why can’t you drink them if you have ARVI? How to restore health if your baby has a stomach ache after a course of treatment? Should I give him probiotics (Bifidumbacterin)? Let's look into these issues, and also find out how Dr. E.O. feels about antibiotic therapy. Komarovsky.
Indications for use
Antibiotics are prescribed to infants only to treat bacterial infections.
Main indications:
- respiratory and otolaryngological diseases - non-viral bronchitis, pneumonia, tonsillitis, otitis media, sinusitis, whooping cough, diphtheria and so on
- gastrointestinal pathologies – salmonellosis, dysentery
- dermatological problems – boils, erysipelas
- urological diseases - cystitis, pyelonephritis and so on
You should not give your child medicine simply because he has a stomach ache or diarrhea. Dr. Komarovsky draws the attention of parents to the fact that all decisions regarding antibiotic therapy for intestinal infection or bronchitis should be made by a doctor. His task is to choose the drug, the method of administration and the duration of administration.
The optimal way to select an antibiotic is to conduct a bacterial culture of sputum, urine or feces. It allows you to identify the culprit of the infection and its susceptibility to medications. But the analysis takes some time, which is why in many cases broad-spectrum antibiotics are prescribed, which act on most bacteria. Why are they dangerous?
Side effects may occur after taking these medications, including:
- dysbacteriosis
- allergy
- irritable bowel
- diarrhea
- decreased immunity
- constipation and so on
Some drugs affect not only the intestines: gentamicin has a bad effect on the kidneys, tetracycline has a bad effect on the liver, and chloramphenicol has a bad effect on hematopoiesis.
Possible negative consequences are not a reason to refuse medications. Bacterial diseases cannot be cured without them. You can minimize side effects by strictly following the doctor’s instructions and taking probiotics (“Bifidumbacterin”).
For infants, doctors try to prescribe the least toxic antibiotics in the form of solutions and suspensions; in rare cases, injection is practiced.
Antibiotics for viral infections
Komarovsky insists that ARVI in children is not treated with antibiotics, since the disease is caused by a virus. Their use is also not permissible as a prevention of complications. Using antibacterial drugs for a runny nose and cough “just in case” increases the risk of secondary infections.
The human body contains many opportunistic microorganisms. They do not cause harm, since some bacterial colonies inhibit the growth of others. If you give a child an antibiotic for ARVI, some of the microbes will die, but those that survived will intensify their activity. As a result, a common runny nose can result in pneumonia.
Komarovsky warns: if bacterial complications have already been added to ARVI, then it is necessary to take antibiotics. They may indicate:
- deterioration of health after improvement
- fever for more than 7 days
- appearance of immature forms of leukocytes in the general blood test
- emergence of new symptoms
Only a doctor can diagnose an infection associated with an acute respiratory viral infection.
Antibacterial agents are often used for bronchitis, which is not always justified.
Komarovsky believes that in many cases, inflammation of the bronchi is a manifestation of ARVI. A bacterial nature may be indicated by purulent sputum, severe intoxication (the child has aching bones, an aching stomach), a temperature that cannot be brought down, and changes in the blood test. With this type of bronchitis, antibiotics are required.
Intestinal problems
One of the side effects of taking antibiotics is irritable bowel disease in a child.
This condition is characterized by:
- flatulence, which causes the baby to have a stomach ache
- diarrhea – frequent liquid green stool with mucus
- constipation - no stool for more than 3 days
Treatment tactics are determined by which symptoms dominate. If a child is breastfed and his stomach often hurts due to increased gas formation, the mother should exclude legumes, cabbage, black bread, kvass, raisins, and grapes from the diet. Potatoes, milk, raw fruits and vegetables should also be limited.
A baby with irritable intestines can be given simethicone-based products (Espumizan), which eliminate flatulence. It is also recommended to take probiotics that normalize microflora, for example, Bifidumbacterin or Bifiform.
If irritable intestines are caused by liquid green feces, then the nursing mother needs to remove “laxative” foods from the menu - cucumbers, prunes, beets, fresh kefir and others. Treatment consists of taking sorbents - Enterosgel, Smecta, probiotics are also indicated.
Constipation can also be treated by adjusting the mother's diet. She should eat fermented milk products, oatmeal, boiled fruits, baked vegetables, and cereals. For bottle-fed infants, fermented milk mixtures can be added to the menu. If changing the diet does not help eliminate constipation, the baby can be given a laxative (lactulose syrup), a glycerin suppository, or an enema.
Microflora disturbance
Dysbacteriosis often occurs after a course of antibiotics. Why is this happening? The active substances of the drugs destroy both harmful microorganisms and beneficial lacto- and bifidobacteria that populate the intestines. As a result, the process of digesting food is disrupted.
Dysbacteriosis in children is manifested by such symptoms as:
- diarrhea - frequent, liquid green stools with mucus and foam
- constipation – rare and very dense stool
- flatulence - increased gas formation, leading to the baby's stomach ache
If the baby is fed breast milk or formula, then dysbiosis leads to the fact that he regurgitates profusely, does not gain weight well and is often capricious. Sometimes a rash appears on the child's body.
How to restore microflora? Komarovsky believes that after stopping taking antibiotics, the balance of beneficial and pathogenic organisms normalizes on its own. During and after an illness, the child must be given plenty of water, especially if he has a stomach ache, liquid green feces (diarrhea) or constipation (infrequent stools).
Because the temperature rises, children eat poorly and lose weight. When the disease subsides, parents try to feed them well. But this is a mistake. The food should be light (vegetable and dairy) and rich in vitamins, and the baby will gain back the lost grams over time.
Normalization of balance
How to help a baby who has dysbiosis? Treatment includes taking sorbents and preparations containing beneficial bacteria. There are various probiotics available today. One of them is “Bifidumbacterin”.
“Bifidumbacterin” is a drug that contains active bifidobacteria, as well as substances necessary to maintain their vital functions. The main indication for taking the drug is dysbacteriosis.
"Bifidumbacterin" is produced in different forms. Children are usually prescribed powder. The dosage regimen for newborns is 1 sachet 2-3 times a day, for babies up to 1 year old – 1 sachet 3-4 times a day. The product must be diluted in milk and given during feeding.
Treatment is carried out for 2-3 weeks. During this period, beneficial bacteria should populate the intestines, displacing opportunistic microorganisms.
If probiotics do not have an effect, and the dysbiosis that accompanies diarrhea, constipation and flatulence does not go away, the child may be prescribed bacteriophages. Their formula includes viruses that do not harm beneficial flora, but only work against pathogenic microbes.
It is advisable to take probiotics in parallel with antibiotics.
Allergy
Antibiotics are one of the reasons why allergies occur. It is impossible to predict in advance the child’s body’s reaction to the drug. Predisposing factors are considered to be poor heredity and food or contact allergies in the baby. These points must be reported to the doctor.
The allergy manifests itself in the form of itchy urticaria or papular rash.
In severe cases, angioedema may develop, which makes breathing difficult, or life-threatening Lyell and Stevens-Johnson syndromes, which are characterized by fever and serious damage to the skin.
These situations require immediate medical attention. Mild allergies after antibiotics are treated with systemic and local antihistamines.
Some doctors practice simultaneous prescribing of antibiotics and antihistamines. Dr. Komarovsky will argue against this. Such actions can lead to the fact that the allergy does not appear immediately and will be very severe.
Sometimes allergies are observed along with symptoms of gastrointestinal disorders such as diarrhea (frequent bowel movements), constipation (hard stool), gas formation. This indicates a weakening of the local immunity of the mucous membranes of the stomach and intestines. The baby may complain that his stomach hurts. A gentle diet, enzymes, sorbents and probiotics (“Bifidumbacterin”) help restore the functioning of the gastrointestinal tract.
Reduced defenses
The intestines play an important role in the functioning of the immune system: it produces protective cells and absorbs useful substances. Disruption of its microflora (dysbacteriosis) or damage to the mucous membranes as a result of taking antibiotics leads to a general weakening of the child’s body. The situation can be aggravated by allergies, rare stools, or, conversely, frequent liquid feces.
How to restore normal functioning of a child’s immune system? Dr. Komarovsky recommends:
- protect your baby from new infections, including acute respiratory viral infections; to do this, for some time after illness you should avoid crowds and walk a lot in the fresh air
- monitor the air in the room where the baby is - the optimal temperature is 18-22 ° C, and humidity is 50-70%
- follow a vitamin-sparing diet and actively water the child so that the body is cleansed of toxins
- carry out gentle hardening
Antibiotics and hyperthermia
Antibiotics do not have an antipyretic effect, but 3-4 days after starting to take them, the temperature should either normalize or decrease, since the active substances of the drug stop the proliferation of bacteria that cause the inflammatory process.
If a child's temperature remains high several days after starting therapy or after its completion, this may indicate:
- incorrect selection of medications or their concentrations
- violation of the regimen - treatment with antibiotics requires strict adherence to the rules of use specified in the instructions; in no case should the dosage be reduced (increased) or multiplicity
- premature termination of use - it is important to complete the full course prescribed by your doctor
- addition of another infection
Sometimes fever is a sign that a child has an allergy. The situations listed above are a reason to consult a doctor.
Antibiotics and lactation
Are antibiotics dangerous for a baby if a nursing mother takes them? It all depends on the type of drug. Penicillins, macrolites and cephalosporins are considered compatible with breastfeeding. If treatment is carried out with their help, lactation can be continued. But these medications can cause side effects for both mother and baby, including:
- allergy
- dysbacteriosis
- diarrhea
- constipation and so on
To prevent them, mothers should take probiotics (Bifidumbacterin, Linex), as well as fermented milk products. In consultation with the doctor, products with beneficial bacteria can be given to the child.
Aminoglycosides, tetracycline, chloramphenicol, lincomycin, metronidazole, some fluoroquinolones and other drugs are prohibited during breastfeeding.
During lactation, treatment of any disease, even simple ARVI, should be carried out under the supervision of a doctor, so as not to harm the baby.
Conclusion
Antibiotics in infancy can only be used as prescribed by a doctor for sore throat, bronchitis, cystitis and other bacterial infections that do not include ARVI. After consuming them, unpleasant consequences may occur - green stools, diarrhea, constipation, death of beneficial microflora populating the intestines, decreased immunity, and others.
You can avoid this if you strictly adhere to the rules for taking medications and take probiotics (Bifidumbacterin) in parallel. Dr. Komarovsky insists on following a light diet, drinking plenty of fluids and walking during the recovery period. If after a course of antibiotics your child has a stomach ache, vomits frequently, or has a high fever, you should consult a doctor.
Source: https://ogrudnichke.ru/lechenie/antibiotiki-grudnichkam-pokazaniya-i-posledstviya-priema.html
Indications for antibiotic therapy
In infancy, it is difficult to avoid all kinds of infections. Some of them are mild and do not require specialized treatment, but in some cases the child may need an antibacterial drug to recover. Only a pediatrician can select antibiotics for an infant after a thorough examination.
It is important to remember that this group of drugs is potent and has a number of unpleasant side effects, so they are prescribed only for strict indications:
In this case, the doctor will prescribe a broad-spectrum antibacterial agent or select a drug taking into account the sensitivity of the microorganisms that caused the disease.
Medicines for babies

The immune system of a newborn child is immature and is not able to fight many pathogenic microorganisms. Antibodies that enter the baby's body with mother's milk have special protection, but sometimes these protective forces are not enough to eliminate the bacterial infection. That is why prescribing antibiotics for infants is the primary task of a specialist when identifying a severe infectious process.
Modern effective drugs approved for use in young children include:
- Penicillin antibiotics – Amoxicillin, Augmentin.
- Cephalosporins – Cefuroxime (Zinnat, Zinacef), Ceftriaxone.
- Macrolide group drugs – Azithromycin (Sumamed), Erythromycin.
- Fluoroquinolones, which are usually prescribed as reserve drugs in severe cases when other antibiotics have not helped - Levofloxacin, Moxifloxacin.
In case of emergency, broad-spectrum medications will be prescribed. But if there is no threat to the patient’s life, it is better to wait and determine the type of microorganisms, as well as its sensitivity to antibiotics. This will help you immediately select the most effective drug and minimize the risk of adverse reactions.
Antibiotics for infants
It's no secret that potent antibacterial drugs help defeat many diseases. That is why many mothers, whenever their baby has a cold, run to the pharmacy and select the medicine themselves. Others, fearing side effects, postpone drug therapy until the last minute. Only a pediatrician can figure out in which case an antibiotic is needed and select the most effective remedy.
Indications for antibiotic therapy
In infancy, it is difficult to avoid all kinds of infections. Some of them are mild and do not require specialized treatment, but in some cases the child may need an antibacterial drug to recover. Only a pediatrician can select antibiotics for an infant after a thorough examination.
It is important to remember that this group of drugs is potent and has a number of unpleasant side effects, so they are prescribed only for strict indications:
- An increase in body temperature above 38 degrees, lasting more than 3 days.
- Severe infectious diseases (acute bronchitis, pneumonia, purulent otitis and sinusitis, tonsillitis).
- Life-threatening illnesses (meningitis).
- Prolonged course of inflammatory processes.
- Changes in the general blood test (increased ESR, leukocytosis with the appearance of young forms of white blood cells).
In this case, the doctor will prescribe a broad-spectrum antibacterial agent or select a drug taking into account the sensitivity of the microorganisms that caused the disease.
Medicines for babies
The immune system of a newborn child is immature and is not able to fight many pathogenic microorganisms. Antibodies that enter the baby's body with mother's milk have special protection, but sometimes these protective forces are not enough to eliminate the bacterial infection. That is why prescribing antibiotics for infants is the primary task of a specialist when identifying a severe infectious process.
Modern effective drugs approved for use in young children include:
- Penicillin antibiotics – Amoxicillin, Augmentin.
- Cephalosporins – Cefuroxime (Zinnat, Zinacef), Ceftriaxone.
- Macrolide group drugs – Azithromycin (Sumamed), Erythromycin.
- Fluoroquinolones, which are usually prescribed as reserve drugs in severe cases when other antibiotics have not helped - Levofloxacin, Moxifloxacin.
In case of emergency, broad-spectrum medications will be prescribed. But if there is no threat to the patient’s life, it is better to wait and determine the type of microorganisms, as well as its sensitivity to antibiotics. This will help you immediately select the most effective drug and minimize the risk of adverse reactions.
Not recommended for use
Prescribing antibiotics and any other potent drugs to infants should be carried out according to strict indications, after a thorough examination, interpretation of test data and establishment of an accurate diagnosis.
There are groups of antibiotics that are contraindicated for use in infants. They are prescribed only in special, severe cases, when other drugs have not helped and the risks of the disease largely exceed the consequences of taking the medicine.
The following are not used in newborns:
- Levomycetin is a toxic drug that, in addition to dyspeptic symptoms and dysbacteriosis, can damage the patient’s bone marrow and cause the most severe pathology, aplastic anemia. This antibiotic is used only in extremely rare cases (typhoid fever, tularemia).
- Aminoglycosides (Streptomycin, Neomycin, Gentamicin) – which are ototoxic and can lead to hearing impairment and even deafness in children.
- Biseptol is a hepatotoxic drug from the sulfonamide group. It is used extremely rarely due to the fact that many bacteria are resistant to the action of its substance.
- Tetracyclines (Tetracycline, Doxycycline) – these medications lead to the destruction of tooth enamel.
For young children, drugs from the fluoroquinolone group are extremely rarely used. Despite their high efficiency and relative safety, they lead to a pronounced side reaction - disruption of the intestinal flora.
Contraindications
Like any other drugs, antibiotics have a number of contraindications for use. They may mean the inability to use the drug or its use with extreme caution (dosage adjustment or prescription of concomitant medications).
Antibiotics should not be prescribed for:
- Increased individual sensitivity to the drug or its components.
- Allergic reactions in infants.
- Intestinal dysbiosis (microflora disturbances may worsen under the influence of medications).
- Infectious mononucleosis and lymphoblastic leukemia are diseases for which some antibiotics are contraindicated.
- Damage to the kidneys and liver - these pathologies require a reduction in dosage and selection of gentle medications.
Before prescribing antibiotics to an infant, the doctor will take a medical history, carefully examine the child and identify possible contraindications to antibacterial therapy.
Side effects
A fragile child's body is more susceptible to the toxic effects of drugs. That is why adverse reactions to antibiotics are recorded in infants much more often than in adults. These include:
- Dyspeptic disorders (indigestion, abdominal pain).
- Intestinal dysbiosis (diarrhea).
- Candidiasis of the oral mucosa.
- Allergic skin rash.
- Liver damage.
- Kidney pathologies.
- Agranulocytosis.
- Disorders of the nervous system.
When treating with antibiotics, it is necessary to strictly adhere to the dosage prescribed by the doctor, which the specialist calculates taking into account the severity of the disease, the age and weight of the baby.
Antibiotic therapy for children
Treatment of infectious diseases in infants has a number of features, which the doctor will definitely tell the mother about at the appointment.
The most important thing is strict adherence to the prescribed dosage and duration of therapy. You should not stop taking the drug before the time specified by your doctor, even if all symptoms disappear completely, as this can lead to a chronic form of the disease and the emergence of antibiotic-resistant strains.
Along with the antibacterial agent, it is necessary to take probiotics and vitamin-mineral complexes in order to restore and maintain normal intestinal flora.
Medicines for infants
Antibiotics for children can be prescribed both in injection form and for oral administration, which is typical for treatment at home. Infants cannot swallow tablets and capsules on their own, so medications are prescribed to them in the form of suspensions, syrups or soluble tablets. Such drugs include:
- Sumamed (Azithromycin) is an antibacterial agent in the form of a suspension, acceptable for use from 6 months of age.
- Zinnat – granules for preparing suspensions.
- Flemoxin Solutab is a soluble tablet with a pleasant fruity taste.
Antibacterial agents are a necessary component of complex therapy for many diseases. You should not ignore the doctor’s prescription and refuse the medicine for fear of its side effects, since the disease causes much more harm to the baby’s delicate body.
elaxsir.ru
Not recommended for use

Prescribing antibiotics and any other potent drugs to infants should be carried out according to strict indications, after a thorough examination, interpretation of test data and establishment of an accurate diagnosis.
There are groups of antibiotics that are contraindicated for use in infants. They are prescribed only in special, severe cases, when other drugs have not helped and the risks of the disease largely exceed the consequences of taking the medicine.
The following are not used in newborns:
- Levomycetin is a toxic drug that, in addition to dyspeptic symptoms and dysbacteriosis, can damage the patient’s bone marrow and cause the most severe pathology, aplastic anemia. This antibiotic is used only in extremely rare cases (typhoid fever, tularemia).
For young children, drugs from the fluoroquinolone group are extremely rarely used. Despite their high efficiency and relative safety, they lead to a pronounced side reaction - disruption of the intestinal flora.
Contraindications

Like any other drugs, antibiotics have a number of contraindications for use. They may mean the inability to use the drug or its use with extreme caution (dosage adjustment or prescription of concomitant medications).
Antibiotics should not be prescribed for:
- Increased individual sensitivity to the drug or its components.
- Allergic reactions in infants.
- Intestinal dysbiosis (microflora disturbances may worsen under the influence of medications).
- Infectious mononucleosis and lymphoblastic leukemia are diseases for which some antibiotics are contraindicated.
- Damage to the kidneys and liver - these pathologies require a reduction in dosage and selection of gentle medications.
Before prescribing antibiotics to an infant, the doctor will take a medical history, carefully examine the child and identify possible contraindications to antibacterial therapy.
Side effects

A fragile child's body is more susceptible to the toxic effects of drugs. That is why adverse reactions to antibiotics are recorded in infants much more often than in adults. These include:
- Dyspeptic disorders (indigestion, abdominal pain).
- Intestinal dysbiosis (diarrhea).
- Candidiasis of the oral mucosa.
- Allergic skin rash.
- Liver damage.
- Kidney pathologies.
- Agranulocytosis.
- Disorders of the nervous system.
When treating with antibiotics, it is necessary to strictly adhere to the dosage prescribed by the doctor, which the specialist calculates taking into account the severity of the disease, the age and weight of the baby.
Antibiotic therapy for children

Treatment of infectious diseases in infants has a number of features, which the doctor will definitely tell the mother about at the appointment.
The most important thing is strict adherence to the prescribed dosage and duration of therapy. You should not stop taking the drug before the time specified by your doctor, even if all symptoms disappear completely, as this can lead to a chronic form of the disease and the emergence of antibiotic-resistant strains.
Along with the antibacterial agent, it is necessary to take probiotics and vitamin-mineral complexes in order to restore and maintain normal intestinal flora.
Medicines for infants
Antibiotics for children can be prescribed both in injection form and for oral administration, which is typical for treatment at home. Infants cannot swallow tablets and capsules on their own, so medications are prescribed to them in the form of suspensions, syrups or soluble tablets. Such drugs include:
- Sumamed (Azithromycin) is an antibacterial agent in the form of a suspension, acceptable for use from 6 months of age.
- Zinnat – granules for preparing suspensions.
- Flemoxin Solutab is a soluble tablet with a pleasant fruity taste.
Antibacterial agents are a necessary component of complex therapy for many diseases. You should not ignore the doctor’s prescription and refuse the medicine for fear of its side effects, since the disease causes much more harm to the baby’s delicate body.
In what cases are antibiotics prescribed to a child? antibiotics for children under one year of age: treatment features
A child’s body cannot cope with some diseases without the help of potent drugs. At the same time, many parents are wary of giving antibiotics prescribed by a doctor to their child. In fact, when used correctly, they will do more good than harm and will contribute to a speedy recovery for the baby.
Antibiotics: definition
Antibiotics are organic substances of semi-synthetic or natural origin that have the ability to destroy microbes or prevent their growth. They cause the death of some bacteria, while for others they remain absolutely harmless. The spectrum of action depends on the sensitivity of the organisms.
Purpose of reception
The action of antibiotics is aimed at combating infectious and bacterial pathologies. In each individual case, the drug should be selected by a doctor depending on the age and condition of the patient.
Such drugs can cause serious side effects such as dysbiosis, neuralgic disorders, and allergic reactions. Most often this happens when the dosage regimen is not followed and medications are taken for a long time.
Many parents think about what antibiotic to give their child for an infectious disease. Self-medication in this case is prohibited. After all, drugs based on tetracyclines and sulfonamides are not used in pediatric practice, and other groups of antibiotics are prescribed according to strict indications.
When do children need antibiotics?
Antibiotics are prescribed to a child if the disease is of bacterial etiology and the body is not able to cope with the pathogen on its own. Treatment of some serious diseases is carried out in a hospital setting, constantly monitoring the reaction of the child’s body without medication. In outpatient (home) settings, “minor” ailments are treated with antibiotics.
In the first days of the disease, it is necessary to monitor the baby’s condition and give the body the opportunity to overcome the disease on its own. At this time, antibiotic therapy is not prescribed. It should be remembered that high fever, cough and runny nose are not yet a reason to use such drugs. Having established the nature of the pathogenic microbes, treatment can begin.
Antibiotics are mandatory for a child to be prescribed for the following diseases:
- Pneumonia.
- Acute otitis (including in children under 6 months).
- Purulent sore throat.
- Acute (purulent) and chronic sinusitis.
- Peritonsillitis.
- Infectious disease of the urinary system.
- Pneumonia.
It is not recommended to treat ordinary bronchitis with antibiotics. Only after confirming the bacterial etiology of the disease, the doctor selects the necessary group of drugs and prescribes a medication dosage regimen.
Treatment of ARVI in children with antibiotics
Acute respiratory infection caused by viruses cannot be treated with antibiotics. Such therapy will only harm the small organism. Professional doctors came to this conclusion. Unfortunately, many parents do not listen to the opinion of qualified specialists and find out from friends what antibiotics children can take for a common cold.
Antibiotics are powerless against viruses until bacteria join them. It is quite difficult to determine this, so control over the course of the disease by a pediatrician is necessary. If the baby returns to a high temperature, the cough intensifies, there is a focus of a chronic illness (tonsillitis, pyelonephritis), a bacterial infection may develop against the background of an acute respiratory infection.
Parents who are unsure whether to give antibiotics to their child even after a doctor’s prescription should realize that in some cases these medications are simply necessary to relieve the symptoms of the disease and speed up the baby’s recovery. After all, an advanced disease is fraught with serious complications.
The effectiveness of antibiotics in diseases of the ENT organs
In childhood, bacterial ENT infections are common and often spread from one place to nearby organs. This is facilitated by their anatomical location. Most often, children exhibit symptoms of tonsillitis, sinusitis, pharyngitis or otitis media.
Having made a diagnosis, the doctor must prescribe antibiotics to the child depending on individual tolerance and the age of the patient.
Typically, drugs from the group of cephalosporins (Cefotaxime, Suprax), penicillins (Flemoxin Solutab, Augmentin), and macrolides (Sumamed, Vilprafen) are used.
Long-term use of drugs will cause addiction (resistance), and the sensitivity of microbes to them will disappear. Therefore, antibiotic therapy is not carried out for longer than 14 days. If the therapeutic effect does not appear after 48 hours, this medicine is replaced with another, taking into account compatibility with the previous one.
Treatment of intestinal infections with antibiotics in children
Children quickly pick up various intestinal diseases, which can be caused not only by bacteria, but also by viruses. When it is necessary to treat a bacterial infection, antibiotics are used: Amoxicillin, Cephalexin. They are prescribed depending on the type of pathogen. Antibacterial drugs and enteroseptics are also used: “Enterofuril”, “Nifuratel”.
Antibiotics for infants
The immune system of newborns is not yet able to repel the “attack” of pathogenic microorganisms. Breastfeeding provides special protection, but if the baby does catch a bacterial disease, the pediatrician is required to prescribe antibiotics.
For children under one year of age, such drugs are usually prescribed if treatment does not give positive results on days 3–5, but in case of serious diseases (meningococcal infection, purulent tonsillitis, chronic pathologies), their immediate use is required).
Harm or benefit?
Modern drugs make it possible to fight bacterial diseases with minimal harm to the small organism. This does not mean that you can give antibiotics to children “just in case.”
Is it possible to do without these drugs? The answer is ambiguous, because some experts are of the opinion that treatment of infants should be carried out without taking antibiotics.
Parents must understand that in this case, serious consequences may develop that will further harm the baby’s health. Therefore, it is necessary to adequately assess the situation and not expose the child to danger.
Antibiotic release forms
Depending on the age of the young patient, antibiotics can be prescribed in the form of a suspension (syrup), tablets or injections. The latter option is used for severe illnesses in a hospital setting.
The most common form is syrup. The bottle always comes with a measuring spoon, which is convenient for calculating the dose of the drug and giving it to the child.
To prepare the suspension, powder is used, which is diluted with water before use.
Whatever form of release the drug is prescribed, it is necessary to strictly adhere to the recommendations of the pediatrician and observe the dosage and duration of antibiotic treatment. It is prohibited to interrupt the medication. You need to complete a full course of antibiotic therapy to completely cure the infection.
Antibiotic nasal drops
Popular in this group of antibiotics are Isofra and Polydex drops. There is absolutely no justification for their use for simple rhinitis, as some parents do. A viral runny nose cannot be treated with such drugs. The ENT specialist should explain exactly when it is necessary to use antibiotics for children.
Treatment of children with drops with antibacterial components is justified only for purulent rhinitis, which occurs quite rarely in children. Sometimes they can be prescribed in the complex therapy of otitis, sinusitis, and sinusitis.
"Polydex" contains a hormonal component, so only a doctor can prescribe this medicine.
Isofra is a safer polymer-based drug, which allows it to be used to treat even newborn babies.
First of all, it is necessary to treat the baby as prescribed by the doctor. Antibiotics are taken by children under the strict supervision of adults.
You cannot use drugs for treatment that have successfully treated the children of friends and relatives. All children are individual, and the disease can have a different etiology.
Only if a bacterial or fungal pathogen is confirmed are these drugs prescribed.
When treating children with antibiotics, it is important to follow the following rules:
- Take only medications recommended by your pediatrician.
- Follow the prescribed dosage.
- Observe the frequency of taking antibiotics.
- Take medications as directed - before or after meals.
- Provide bed rest for the baby.
- Put your newborn baby to the breast more often.
- Older children should be given plenty of fluids.
- If there is no improvement or an adverse reaction occurs, you should inform your doctor.
- Complete the entire course of treatment, do not interrupt in advance.
Consequences of taking antibiotics
Drugs with antibacterial effects can not only cure an infection, but also cause harm to a small organism. First of all, parents are afraid of subsequent treatment for dysbiosis.
Indeed, after taking antibiotics, a child may encounter this unpleasant disease, which causes a disturbance in the intestinal microflora, constipation, diarrhea, flatulence, and a feeling of bloating.
Experts say that if you follow the recommendations, the risk of the disease is significantly reduced.
Antibiotic medications can cause an allergic reaction in children in the form of skin rashes (dermatitis), attacks of nausea, dizziness, burning in the nose (when using drops), increased heart rate, candidiasis on the oral mucosa, and anaphylactic shock.
To prevent the development of side effects, it is necessary to follow the instructions for use of the medicine and follow the prescription of the attending physician when using prescribed antibiotics for the child.
If these symptoms occur, you should urgently seek medical help.
Indications and subtleties of administering Ceftriaxone to a newborn

Ceftriaxone is prescribed to newborns only with a confirmed bacterial infection (for example, staphylococcal). The most common indications are pneumonia, pyelonephritis, tonsillitis, suppuration of the umbilical wound. Dose per day – 20-50 mg per 1 kg of weight for a child up to 2 weeks, from 14 days to a year – 20-80 mg/kg. It is administered intravenously 1 time per day in a dropper or as a jet injection. For convenience, a venous catheter is placed in the baby. If injections into a vein are not possible, injections are made into the buttock.
The use of the drug is prohibited for jaundice and increased blood bilirubin. In hemolytic disease of newborns, Ceftriaxone is dangerous due to the displacement of bile pigment from the protein complex and the development of bilirubin encephalopathy (brain damage). The most common complication in a child is intestinal dysbiosis.
Brief overview of these drugs
The choice of remedy will depend on the type of infection, the severity of the disease and the age of the baby. Still, it is useful for parents to know which antibiotics are used for the most common childhood diseases:
- Amoxicillin is used in the therapeutic treatment of otitis, cystitis, urethritis, pneumonia, sinusitis, tonsillitis and pharyngitis. Children under two years of age are prescribed a dose of a quarter teaspoon.
- Zinacef is prescribed as an injection for similar diseases.
- The doctor recommends Sumammed Forte for the same ailments. The child should be given it once a day with plenty of fluids. The drug is contraindicated in infants under six months of age.
- Zinnat is used by pediatricians for diseases of the ENT organs, upper and lower respiratory tract, and genitourinary infections. Not prescribed for children under 3 months.
- Flemoxin Solutab can be used in the treatment of infants and children under 1 year of age. This remedy is quite effective in the treatment of infections of the ENT organs, soft tissues, gastrointestinal tract and genitourinary system.
- Augmentin has indications similar to Amoxicillin and Amoxiclav, but it is contraindicated in children under three months.
- Ceftriaxone has a broad spectrum of action and is used in the treatment of children when other antibacterial agents are ineffective. It comes in the form of injections, which are quite painful.

- To combat coccal infections and clostridia, Cephalosporins are used: Suprax, Zinnat or Macrolides: Sumammed, Macropen, as well as Benzylpenicillin and Bicillin.
- Modern cephalosporins (Cedex, Ceftriaxone) and some penicillins (Augmentin) successfully combat gram-positive bacteria.
- Antibiotics that destroy gram-negative bacilli: Polymyxins and Cephalosporins.
It is difficult to navigate such a huge selection without the help of a qualified specialist. And it is simply impossible to assess the advantages and disadvantages of each of them without certain knowledge. Therefore, the choice of remedy should be entrusted to a specialist, and the responsibilities of parents include compliance with the dosage and regimen.
When is Ceftriaxone prescribed to newborns?
It is recommended to administer Ceftriaxone to a newborn (from birth to one year) after confirmation of the diagnosis.
It is needed only for bacterial infections of organs and systems:
- blood (sepsis); Omphalitis
- vascular membranes of the brain (meningitis);
- heart valves (endocarditis);
- lungs (pneumonia);
- ENT organs (otitis media, sinusitis, tonsillitis);
- abdominal cavity (peritonitis - inflammation of the peritoneum, enterocolitis);
- biliary tract;
- umbilical wound (omphalitis);
- digestive system;
- bones and joints (osteomyelitis, arthritis);
- skin and soft tissues (abscess, boil, phlegmon);
- wounds after surgery or injury;
- kidneys and urinary tract (nephritis, pyelitis);
- congenital syphilis, gonorrhea.
The antibiotic has no effect on viruses and fungi. Ceftriaxone can be recommended only for severe or moderate cases of the disease; for mild cases of the disease, other drugs are used in the form of a pediatric suspension.
And here is more information about whether Ceftriaxone will help against staphylococcus.
Pre-appointment examination
Before starting antibiotic treatment, it is important for a child to:
- conduct a pediatric examination;
- perform blood tests to determine the pathogen and its sensitivity to Ceftriaxone;
- donate blood biochemistry with kidney and liver tests;
- in the first days of life, additionally examine: bilirubin level, acid-base status, total protein and albumin content.
If there are any signs of allergies (to food or to medications in the past), the child is given a skin test to determine the tolerance of the antibiotic, and if intramuscular administration is necessary, the reaction to the solvent (usually lidocaine) must be known.
Skin test
Features of antibacterial therapy in premature newborns
AND
Infectious and inflammatory diseases are the most common pathology in children of the neonatal period, which is explained by the uniqueness of protective mechanisms at this stage of ontogenesis. The most pronounced deficiency of humoral and cellular immunity, immaturity of the barrier functions of the skin and mucous membranes in children born prematurely. In the structure of diagnoses in departments of the second stage of nursing premature babies, the proportion of purulent-inflammatory diseases approaches 80%, with the majority of diseases being so-called minor infections - pustular rashes, omphalitis, dacryocystitis, otitis media; In 1% of children, serious inflammatory diseases are detected (cellulitis and pemphigus of newborns, osteomyelitis, meningoencephalitis, pneumonia, sepsis).
In recent years, the problems of infectious pathology in immature children have become particularly relevant due to changes in the characteristics of both macro- and microorganisms, which affected the course of the infectious process. The course of background conditions has become more severe, creating favorable conditions for the manifestation and progression of infection - these are perinatal brain lesions, congenital malformations, pneumopathy; Moreover, the achievements of modern resuscitation and intensive care make it possible to ensure the survival of even children with extremely low body weight who have suffered severe asphyxia. In turn, resuscitation measures, primarily long-term mechanical ventilation and catheterization of the great vessels, create conditions for microbial aggression. One of the important factors contributing to bacterial contamination and aggravation of the course of bacterial infections is the presence of a mixed viral-bacterial intrauterine infection. Intrauterine parasitic and viral infections (the so-called TORCH syndrome) are the main cause of mortality in the neonatal period in 13–45% of cases. A specific infection transferred in utero sharply disrupts the child’s defense mechanisms, which contributes to the occurrence and rapid course of intranatal and postnatal bacterial infections.
Modern etiology of pathogens
In the etiological structure of pathogens of bacterial infections in premature infants 10–15 years ago, there was an increase in the proportion of gram-negative flora (Klebsiella, Proteus, Pseudomonas). However, in subsequent years, again among the etiological agents of local purulent-inflammatory lesions, the first place is occupied by gram-positive flora
(staphylococci, streptococci).
Premature babies are characterized by a combination of microorganisms
isolated from various foci (for example, Staphylococcus aureus and Staphylococcus epidermidis are sown from a purulent focus, Escherichia coli and staphylococci are sown from feces), as well as
a change in the leading pathogens during treatment
(the initial agents of inflammation are suppressed, others take their place bacteria, often in combination with fungi).
Predominantly antibiotic-sensitive strains of pathogens circulate among the population (V.K. Tatochenko), and in hospitals children are infested with predominantly resistant strains (nosocomial flora), since opportunistic and saprophytic microorganisms are repeatedly passaged on weakened immature newborns and their selection occurs under the influence therapy (G.V. Yatsyk, I.V. Markova). In addition, resistant strains (Klebsiella, Streptococcus B) are transmitted to newborns from sick mothers.
Specifics of antibiotic pharmacokinetics
In newborns, the pharmacokinetics of any drug differs significantly from that in older children; This applies to the greatest extent to immature (premature) newborns. The immaturity of the excretory function of the kidneys and liver enzyme systems seems extremely important
These features are primarily characteristic of very premature infants weighing less than 1500 g. In addition,
the immaturity of other organs and systems
(gastrointestinal tract, nervous system, respiratory organs), as well as general
metabolic lability
, impose individual differences on the pharmacokinetics of antibiotics in premature infants. features predetermining a high risk of unwanted side effects of antibacterial therapy.
A general feature of the pharmacokinetics of any drugs in premature infants is its slowdown, which contributes
to the accumulation of drugs and affects the choice of dose (reducing it by 1/3–1/4), routes and frequency of drug administration.
At the same time, the increased permeability of natural barriers
(skin and mucous membranes) facilitates the absorption of many medications. Currently, studies are being conducted on the circadian rhythms of the pharmacodynamics of various drugs, but there are practically no such studies regarding antibiotics in premature infants.
Indications and choice of antibiotic
An absolute indication for prescribing antibiotic therapy to a premature newborn is the presence of any infectious-inflammatory process, including so-called minor infections, for example, non-spread pustular skin lesions, purulent conjunctivitis, otitis (including catarrhal otitis). Only in rare cases of a mild course of uncomplicated acute respiratory viral infection (rhinopharyngitis) is an antibiotic not prescribed - and then only in children with a relatively favorable background (slight degree of prematurity, no anamnestic indications of intrauterine infection, mild perinatal encephalopathy).
An absolute indication for antibiotic therapy for a premature newborn is the presence of any infectious-inflammatory process, including so-called minor infections, for example, non-spread pustular skin lesions, purulent conjunctivitis, otitis (including catarrhal otitis). Only in rare cases of a mild course of uncomplicated acute respiratory viral infection (rhinopharyngitis) is an antibiotic not prescribed - and then only in children with a relatively favorable background (slight degree of prematurity, no anamnestic indications of intrauterine infection, mild perinatal encephalopathy).
The controversial issue of the so-called prophylactic use of antibiotics
in low birth weight premature babies at risk for intrauterine and intrapartum infection (sick mother, long anhydrous period, etc.), as a rule, it is decided in favor of prescribing an antibiotic, as well as in cases of so-called non-infectious pneumopathy. Conditionally “preventive” can also include the prescription of an antibiotic to “cover up” hormonal corticosteroid therapy and certain interventions (catheterization, blood transfusion, etc.).
The choice of antibiotic for a premature baby is a crucial moment that largely determines the effectiveness of treatment. When choosing a drug, the following factors should be considered:
• type of pathogen
(at the beginning of treatment, often only suspected) and its strain;
• pathogen sensitivity
(also at the beginning of treatment - expected, 2-3 days after receiving the results of bacteriological tests, adjustments may be made to the therapy). In recent years, an opinion has been expressed that the sensitivity parameters of microbes in vitro do not always coincide with those in vivo and there is no need to strictly follow them when prescribing drugs;
• localization and severity of the infectious process
(for mild local lesions, oral administration of the drug is possible; for severe ones, as a rule, a combination of oral and parenteral drugs);
• accompanying conditions and premobid background
(preference for parenteral drugs in severe dysbiosis or intravenous administration in extremely low birth weight children with undeveloped muscle tissue).
All antibiotics can be divided into 2 groups - first choice drugs
prescribed when there is no reason to think about the drug resistance of the flora (semi-synthetic penicillins, first generation aminoglycosides, first generation cephalosporins);
second-choice drugs
are aimed at overcoming resistant strains (aminoglycosides and cephalosporins of the III–IV generation, modern macrolides).
There are also third-choice drugs (or reserve drugs
) used for extremely severe forms of diseases with multidrug-resistant flora (carbapenems).
In premature babies, second-choice drugs are generally immediately used: the use of first-line antibiotics is ineffective and only helps to delay the manifest manifestations of the infectious process and masks clinical symptoms. In children of the neonatal period, even for health reasons, drugs with high toxicity (fluoroquinolones) should not be used.
Scheme 1. Acceptable combinations of antibiotics in premature infants with simultaneous use (G.V. Yatsyk)
Features of antibiotic dosage
Dosages of antibiotics used in neonatology for premature infants and the frequency of their administration are presented in Table. 1 (G.V. Yatsyk, 1998) The general principle of dose selection for a newborn child is a larger amount of the drug per 1 kg of body weight compared to older children
– persists in premature babies.
This is due to the higher percentage of water in the newborn’s body and the larger relative surface area of the body. The dosages of antibiotics used in neonatology for premature babies and the frequency of their administration are presented in Table.
1 (G.V. Yatsyk, 1998) The general principle of selecting a dose for a newborn baby remains the same for premature babies. This is due to the higher percentage of water in the newborn’s body and the larger relative surface area of the body. Combination therapy
Combined antibacterial therapy in premature infants should be carried out with great caution; a simultaneous combination of 2 (very rarely - 3) antibiotics is used only in children with severe purulent-inflammatory processes (primarily sepsis) caused by mixed flora. Acceptable combinations of antibiotics are presented in table. 2 and in diagram 1 (data from N.V. Beloborodova).
Routes and frequency of administration of antibiotics to a premature baby
Due to the high permeability and vulnerability of the gastrointestinal mucosa in immature newborns, as well as the risk of developing dysbiosis and necrotizing ulcerative enterocolitis, oral antibiotics have been used to a limited extent. In addition, most infectious diseases in premature infants require more powerful therapy due to the severity of their condition. In recent years, quite effective antibacterial and antifungal drugs for oral use have appeared (macrolides, amoxicillin/clavulanate, etc.). In addition, the extremely negative impact of painful irritations on infants has been established, which makes it necessary to limit intramuscular and intravenous injections
.
In newborns (especially premature babies), the half-life of drugs is increased due to the immaturity of the kidneys and liver. Therefore, the frequency of administration of most drugs does not exceed 2 times during the day.
(except penicillins); Long-acting drugs (roxithromycin, ceftriaxone), which can be used once, remain especially popular in neonatology. Some researchers (N.V. Beloborodova, O.B. Ladodo) suggest administering most parenteral drugs (including aminoglycosides, cephalosporins) once - intravenously or intramuscularly.
Duration of therapy
The duration of antibacterial therapy and the sequence of antibiotics used in a premature baby are determined individually; they depend on the effectiveness of the initial course of antibacterial therapy, which is assessed using traditional clinical and laboratory parameters. As a rule, premature infants with moderate infectious processes (omphalitis, pneumonia, otitis, etc.) are given two consecutive courses of antibiotics (the second course taking into account the sensitivity of the microflora), each lasting 7–10 days. For severe diseases (meningitis, osteomyelitis, sepsis), at least 3–4 courses of antibiotics are usually used (or 2–3 courses; in the first, a combination of antibiotics, usually an aminoglycoside and a III–IV generation cephalosporin).
Side effects and their prevention
The most common undesirable side effects of antibacterial therapy in premature newborns are caused by suppression of symbiont microflora and, as a consequence, colonization of the body by opportunistic saprophytes. In this regard, even after a short course of antibacterial therapy, premature infants may develop dysbiosis
– candidiasis of the skin and mucous membranes, intestinal dysbiosis.
toxic
(idiosyncrasy-type) and
allergic reactions
to antibiotics are observed in premature infants
Prevention of complications of antibacterial therapy begins with its correct selection and careful individual monitoring. Along with prescribing antibiotics, the child must be prescribed antifungal agents.
(levorin, fluconazole, amphotericin B) and
agents that restore intestinal microflora
(bifidum-bacterin, etc.);
Moreover, the use of the latter continues for at least a week after the end of the course of antibiotics. In order to reduce the load of antibiotics on the immature body of a premature baby, in recent years attempts have been made to combine antibacterial therapy with agents that enhance nonspecific protection : immunoglobulins, laser therapy (the use of low-intensity laser radiation on great vessels for the purpose of immunostimulation), and metabolite correction.
Contraindications to the administration of Ceftriaxone to a newborn child
The main contraindications for prescribing Ceftriaxone to a newborn child include:
- intolerance to this antibiotic or drugs from the group of cephalosporins, penicillins or any of the beta-lactam medications (a drug allergy to an unknown drug requires a skin test);
- prematurity, if the duration of life and intrauterine development is less than 41 weeks;
- up to 28 days of life with jaundice, increased bilirubin levels, high blood acidity (acidosis), decreased albumin;
- if necessary, simultaneous administration of calcium solutions.










