The development of a new life begins from the moment the female egg is fertilized by male reproductive cells - sperm. This is how nature intended. However, the realities of our lives are such that a simple natural process can be disrupted. For example, a woman’s lack of ovulation may become an obstacle to conception. If there is no ovulation, then, accordingly, there is no egg ready for fertilization.
A similar phenomenon is called anovulation (lack of ovulation), and irregular ovulation also occurs. These situations are classified as endocrine infertility. The formation of pathology occurs at the hypothalamus-pituitary-ovary level, and the cause of failure can be various diseases of the endocrine or reproductive systems.
In this case, the procedure for stimulating ovulation comes to the rescue in the fight against endocrine infertility in women.
Menstrual cycle
This term is very easy to explain. If a woman does not experience maturation of her eggs, then it is necessary to eliminate this obstacle that is preventing conception.
Activation of folliculogenesis (formation and maturation of eggs) is based on processes natural to the body. The menstrual cycle of each woman is individual, but has a certain similar rhythm, which is regulated by the coordinated functioning of the endocrine glands (hypothalamus-pituitary-ovaries).
In the first phase of the monthly cycle, which is called follicular, the formation and maturation of so-called “bubbles” - follicles - occurs. They contain the egg.
The follicular phase begins on the first day of menstruation (menstruation). Phase 1 of the cycle ends with ovulation, that is, the release of a mature egg from the dominant follicle, on day 14. However, the end of the follicular phase is a purely individual criterion, which depends on the duration of the menstrual cycle. So, with a cycle of 28 days, ovulation occurs exactly on the 14th day, but with a longer or shorter cycle (21 or 32 days), the maturation of the egg shifts in time and can occur on the 8th or 17th day.
Simultaneously with the growth of follicles, changes occur in the uterus. So, on the first day of the follicular phase, the “unusable” endometrium is rejected, the inner surface of the uterus is cleansed and prepares to grow a new layer.
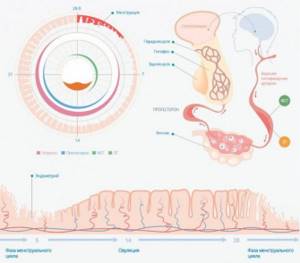
In the first phase, the predominant hormone is estrogen, under the influence of which a new mucous layer of the uterus is formed - the endometrium. Such changes are necessary for successful conception, the likelihood of which increases as ovulation approaches. If, simultaneously with the growth of the dominant follicle, the endometrium does not increase, then with successful fertilization, the fertilized egg will have nowhere to gain a foothold, and accordingly, such a conception will not end successfully.
By the time the Graafian vesicle, the strongest and most mature follicle, forms, the woman’s body begins to produce luteinizing hormone, which continues for up to 3 days. The pulsating rhythm of hormone release leads to rupture of the follicle and the release of the egg (ovulation itself). At the same time, estrogen levels decrease.
The Graaffian vesicle itself degenerates into the corpus luteum and begins to produce progesterone, as well as estradiol and androgens. These hormones are necessary for the attachment (implantation) of a fertilized egg. In the event of conception, the corpus luteum produces the necessary hormones until the formation of the placenta, which then independently produces progesterone and estrogen.
If conception does not occur, then the functioning of the corpus luteum fades away. Swelling of the endometrium is observed, and then menstruation and a new menstrual cycle begin.
These, in a nutshell, are the monthly changes in a woman’s body. With the development of anovulatory infertility, this mechanism is disrupted. This happens, most often, due to hormonal imbalance, when the production and concentration of certain female sex (and not only) hormones is disrupted.
Relaxation to stimulate ovulation
Since disorders of the hormonal system often occur against the background of stress, they need to be treated with all available relaxing methods.
If you don’t have enough time to go to the spa, you can do the same procedures at home. For example, mud therapy. They say that regular procedures help in the treatment of the female genital area and have a positive effect on hormonal levels. Sanatoriums even produce mud for mud tampons. They are used in the first phase of the cycle and warmed up before being used for their intended purpose.
What would a relaxing bath be without aromatic oils? Moreover, there are oils that stimulate the production of estrogen. These include sage, anise, basil, vetiver, lavender, cypress, rose, jasmine, sandalwood. These same oils can be used to enrich massage creams. It is especially useful in the middle of the cycle, before the expected date of ovulation.
An unusual, but allegedly effective way to stimulate ovulation is to take baths with kelp. It is sold at the pharmacy. First, the kelp is steamed in hot water and then added to the bath. And the same goes for plantain roots. A glass of dry roots is poured with hot water, infused and then added to the bathing water.
Method three:
Purposes of stimulation
Stimulation for conception has several goals.
- Firstly, it is the induction (activation) of ovulation.
- Secondly, simultaneously with the growth of follicles, the uterus is stimulated in preparation for conception.
This is explained by the choice of drugs used for stimulation, the effect of which enhances the functioning of the reproductive organs. Under the influence of drugs, the dominant follicle matures and, accordingly, the endometrium enlarges, which prepares to receive a fertilized egg. That is, the main principle of stimulation for conception is the forced creation of conditions for the formation of natural processes in the body.
The choice of treatment regimen depends on the results of the examination, which will give a full assessment of disorders and disruptions in the endocrine system. A mandatory condition will be confirmation of the absence or failure of ovulation. To do this, a procedure for measuring basal temperature is prescribed, which is not always convenient for a woman and is quite uninformative, since it is impossible to assess the growth of the endometrium.
The most informative method will be ultrasound monitoring of folliculogenesis and the degree of endometrial development for at least 3 menstrual cycles, based on the conclusion of which a verdict is made on the need to intensify ovulation.
Features of ovulation after tubectomy
Sometimes the process of maturation of the egg on the side of the removed tube does not occur. This happens due to complications after surgical termination of an ectopic pregnancy. Usually the culprit is an endocrine disruption that requires professional correction. Due to hormonal imbalance, follicles may begin to develop backwards, and ovulation does not occur after tube removal. The egg can be released into the peritoneum, “live” for 2 days and be destroyed there. It is able to float along the abdomen, reach the intact tube and pass through it into the uterus. This is the most favorable outcome for the release of the egg cell. Painful ovulation after an ectopic pregnancy can be accompanied by weakness in the body, slight nausea, and dizziness. Sometimes there is mucous discharge from the vagina with bloody impurities, which happens due to surgery. Subsequent ovulations should not be accompanied by similar phenomena.
Diagnostics
It is quite natural that before prescribing treatment it is necessary to undergo an examination.
The main examination will be aimed at clarifying the woman’s hormonal status, the condition of the reproductive organs, and excluding diseases of organs and systems. The scope and list of necessary procedures is determined by the treating specialist. Mandatory activities are:
- Blood tests for hormones: FSH, LH, prolactin, testosterone, thyroid hormones and others.
- Ultrasound examination of the pelvic organs to detect changes in the uterus and/or tubes. It is possible to conduct studies aimed at determining the patency of the fallopian tubes (hysteroscopy or laparoscopy).
- Blood tests for TORCH infections, HIV.
- Vaginal smear for flora and degree of purity.
- Consultation: mammologist, endocrinologist, therapist.
- For the spouse: examination for the presence of sexually transmitted infections; spermogram.
After the research, ultrasound monitoring of ovulation is prescribed, lasting at least three menstrual cycles.
In the case where a man’s spermogram shows a poor result, there is no need to stimulate women to conceive. Since no stimulation scheme will allow a couple to conceive. Every effort must be made to improve the qualitative and quantitative characteristics of the spouse’s sperm.
Reasons for lack of ovulation
Sometimes after interruption of an ectopic gestation, the ovulation process does not occur. The reasons include the following circumstances.
- Pathological. Sometimes, with obesity or exhaustion, hormonal balance is disrupted. Inflammatory lesions also develop due to poorly performed surgery.
- Physiological. When an ectopic pregnancy occurs in a woman after 40 years of age, the absence of ovulation can be considered a signal of the onset of early menopause.
The absence of the ovulatory process is also influenced by the number of tubal gestations. If this happens for the first time, the egg cell will begin to mature in 1-2 months, when the body has fully recovered and there are no associated pathologies. Normally, even girls under 30 have “empty” cycles 1-2 times a year. Then the egg does not mature. The number of such cases increases after 30 years. The phenomenon becomes more frequent when one tube was removed due to ectopic gestation.
Contraindications
As with most medical procedures and manipulations, when prescribing stimulation, contraindications should be taken into account:
- Obstruction of the fallopian tubes.
- Inflammatory diseases of the reproductive organs.
- Genetic and/or chromosomal pathologies.
- Systemic chronic diseases.
- Venereal diseases.
- Age over 36 years.
Some contraindications are relative and can be eliminated after treatment.
In what cases is the pipe removed or ceases to function?
The most common reason for removal of part of the reproductive organs is ectopic pregnancy .
In rare cases, doctors are able to preserve the fallopian tubes by removing the embryo without damage.
However, its preservation may lead to a repeat ectopic pregnancy, so medical opinions on this matter are very ambiguous.
Quite often it is still removed. But not only an ectopic pregnancy can cause removal.
Also, a similar operation is performed for inflammatory processes and infectious diseases that have a negative impact in the form of the formation of adhesions and obstruction.
This part of the appendages has fairly thin walls, which are quite easy to damage. They cannot be restored, therefore, in most cases, they are deleted.
The main reasons for pipe removal:
- Ectopic pregnancy;
- Inflammation in the tissues of the tubes often leads to the need to remove them. Complete or partial - depends solely on the complexity of the inflammatory process;
- Adnexitis. This disease is an inflammation of the uterine appendages caused by pyogenic bacteria. If not detected in a timely manner, there is a high risk of infertility;
- Appearance of liquid;
- Changes in the structure of the constituent appendages.
Specifics of the procedure
The induction of folliculogenesis is based on three main principles:
- A thorough examination of the patient to identify all the causes of anovulation.
- Necessary preparatory therapy prescribed based on the results of the examination.
- Individual selection of stimulation schemes based on the results of the studies.
Preparation for conception begins already at the second stage, when the woman receives the treatment she needs. In some cases, after completion of treatment, pregnancy occurs immediately, since all pathological barriers that interfere with the maturation of eggs are eliminated.
The basis of preparation for conception is the stimulation of the mucous uterine layer - the endometrium. It is important to be able to grow the required thickness of the endometrium, since if the thickness is not sufficient, implantation of the fertilized egg will not occur.
To stimulate the uterus, drugs containing both estrogens and gestagens are used (Proginova, Divigel, Utrozhestan, etc.). Such drugs are prescribed from days 2-5 of the menstrual cycle to day 14. Approximately on the 10-11th day of the cycle, you need to start visiting the ultrasound room; this is necessary to monitor the development of the endometrium and folliculogenesis. At the same time, drugs are prescribed that improve follicle maturation (gonadotropic hormones, clomiphene citrates).
If ultrasound monitoring shows good conditions for conception, the woman is prescribed a hCG-stimulating drug that induces ovulation. One day before the injection and within two days after the administration of the drug, the spouses need to begin active actions, that is, have unprotected sexual intercourse.
After stimulation and sexual intercourse, the patient is prescribed Duphaston to help implant the fertilized egg.
Stimulants
Stimulation of ovulation is the most common method in the treatment of infertility.
Since the use of this technique does not exclude certain risks (hyperstimulation, multiple pregnancies, etc.), and also taking into account the cost of the procedure and the psychological impact on patients, a preliminary examination is always necessary before prescribing ovarian stimulation.
With this examination you can:
— identify contraindications to stimulation;
-prescribe preliminary therapy (for example, estrogen therapy);
-select the desired regimen and dosage, thereby creating optimal conditions for a successful attempt with minimal risk to health.
Necessary examinations before starting ovarian stimulation:
1.Checking the patency of the tubes ( HSG , Echo- HSG , laparoscopy)
A necessary examination before any stimulation, regardless of the diagnosis.
2. Compatibility test
This analysis will allow, in case of incompatibility, to prescribe stimulation with artificial insemination. In the absence of ovulation, the test is performed during the first stimulation.
3. Spermogram
4. Hormonal study
This examination must be carried out at the very beginning of the cycle - before the 5th day of the cycle. Preferably on day 3.
• FSH
It is unthinkable to start stimulation without testing for the FSH hormone, since it is the best indicator of ovarian reserve. When it is low (<2), then there may be a problem at another level (hypothalamus, pituitary gland). When the level is slightly elevated (from 10 to 15), this indicates the onset of ovarian resistance (resistance) and in such cases it is necessary to carry out preliminary treatment (estrogen therapy, GnRH agonists) before starting stimulation. When the level is clearly too high (>15), stimulation is contraindicated. Normal levels (from 2 to 9) allow you to select normal doses of gonadostimulants.
• LH
LH testing is also necessary. When it is low (<2), it indicates a deficiency in hypothalamic or pituitary activity and the use of FSH stimulants is contraindicated. High levels are indicative only in relation to FSH: if the difference is greater than 1.4 (FSH greater than LH), this indicates a potential good ovarian response, if it is below 0.5, a possible weak response.
• Prolactin
Women are often mistakenly diagnosed with Hyperprolactinemia and given unnecessary treatment that has a detrimental effect on follicular development.
When taking blood for this hormone, you need to take into account its susceptibility to the patient’s stress and even to reactions such as fear of injections or needles. In this case, prolactin levels may jump. To prevent this from happening, you need to find out from the laboratory whether they follow the rules necessary for testing for prolactin. As a rule, the absence of galactorrhea indicates normal prolactin levels.
• Estradiol
The indicators of this hormone are also informative in the prognosis of the ovarian response. A high level indicates accelerating folliculogenesis, which means the beginning of ovarian depletion. Despite this, publications on this topic are contradictory and experience shows that there is no clear relationship between estradiol and ovarian response.
• Androgens
There is absolutely no need to systematically check androgen levels before starting stimulation. Only if there are clinical signs of hyperandrogenism, a testosterone test is done. If it is too high, then tests are done for 17-hydroxyprogesterone, DHEA-S to identify the cause: adrenal glands or ovaries.
5. Assessment of ovarian reserve
Before ovulation stimulation begins, the so-called ovarian reserve is usually determined, that is, the reserve of functional activity of the ovaries. This is especially important for women over 35 years of age and for women with unexplained infertility (infertility of unknown etiology). Based on these tests, it is preliminarily assessed whether the ovarian response will be poor or not.
• Measuring the concentration of FSH, estradiol.
On days 2-3 of the menstrual cycle, the levels of the hormones FSH, LH and estradiol are assessed. An increase in their concentrations is unfavorable and indicates a poor ovarian response to stimulation.
• Clostilbegit test.
On day 3 of the cycle, the FSH level is determined. After this, clostilbegit is prescribed 100 mg (2 tablets) per day from days 5 to 9 of the cycle. On day 10 of the cycle, FSH levels are measured again. If it rises significantly, this indicates a hidden decrease in ovarian reserve, which cannot be determined by simply measuring the level of this hormone.
• Test using GnRH agonists.
The patient receives diferelin or decapeptyl 0.1 mg subcutaneously. Estradiol levels are measured before and after this procedure. An increase in estradiol concentration indicates a high probability of pregnancy.
6. Ultrasound Research
Ultrasound examination at the beginning of the cycle until day 7 is a necessary examination before starting stimulation. In addition to detecting abnormalities in the lower pelvis, ultrasound will determine the type and type of ovaries (area, stroma density, number and location of follicles), and the thickness of the endometrium. After this study, the ovaries can be classified as:
Micro-polycystic: area > 8 cm2, 10 or more small follicles in each ovary, located along the periphery, dense stroma. This type of ovary tends to respond very strongly to stimulation with FSH, so start with low doses.
Multi-follicular ovaries: Many follicles 6 to 8 mm in diameter in each ovary with a homogeneous arrangement of follicles, normal stroma. This type of ovary is usually observed with a diagnosis of high amenorrhea and is accompanied by a high risk of multiple pregnancy.
Exhausted ovaries: area less than 4 cm2, less than 4 follicles per ovary, a follicle with a diameter of 10 mm or more is observed on days 5-6 of the cycle. Such ovaries respond poorly to stimulation and it is necessary to undergo preliminary therapy (estrogenic). Doses of FSH should be quite large.
Normal ovaries: They are not included in the parameters of all the types of ovaries described above and respond normally (average) to stimulation.
Drugs used to stimulate ovulation.
1. Based on human menopausal gonadotropin (HMG). (menogon, pergonal, metrodin, menopur).
The active component of drugs in this group is obtained by processing the urine of women in menopause (therefore the second name is urinary gonadotropins). This series is characterized by a large percentage of impurities and contains both hormones - LH and FSH at a dosage of 75 IU (international units). Despite their low activity compared to more advanced drugs, these drugs are widely used, since they are more preferable in some situations, and they are also much cheaper than recombinant drugs.
2. Based on the recombinant hormone FSH. (puregon, gonal-F).
These drugs are called recombinant because they are synthesized in the laboratory thanks to the achievements of genetic engineering. The structure of the gene encoding the FSH hormone was deciphered, after which this gene was synthesized and introduced into a Chinese hamster, which led to the active production of the hormone by these animals. The drugs in this series are distinguished by the highest degree of purification - 99%, have virtually no LH activity and are very close in their effect to natural FSH. These medications are produced in dosages ranging from 37.5 to 200 IU.
3. Based on recombinant LH hormone.
The production mechanism is the same as that mentioned above, it was developed recently and is currently just beginning to be introduced into clinical practice.
4. Human chorionic gonadotropin (hCG). (decayed, prophase, choragon).
Preparations based on this hormone are needed for the final maturation of eggs, as well as to ensure ovulation. Typically, hCG is prescribed in doses of 5–10 thousand IU when the follicle reaches 18–24 mm.
5. Clomiphene citrate (clostilbegit, serofen, clomid).
A classic drug that belongs to the class of anti-estrogens. Traditionally prescribed in a dosage of 50-150 mg from days 5 to 9 of the cycle. Clostilbegit has a pronounced anti-estrogenic effect, due to which it can not only not help, but also harm. Even according to the instructions, it is not recommended to take Clostilbegit more than 5-6 times in a lifetime. The consequences of drug abuse can be quite dire, including “early ovarian failure” (or “early menopause”).
6. Gonadotropin-releasing hormone agonists.
These drugs are used to prevent the so-called spontaneous LH peak, that is, a sharp increase in the concentration of the hormone LH, which causes ovulation. In addition, the use of GnRH agonists promotes better and synchronous growth of follicles, increasing the likelihood of implantation. Conducted studies of stimulation cycles with and without GnRH agonists have shown that their use enhances the ovarian response, leads to the production of a large number of high-quality embryos and, accordingly, increases the likelihood of pregnancy. The beginning of taking agonists is accompanied by a short-term increase in LH levels. They are used both in depot form and as daily injections.
7. Gn-RH antagonists.
One of the main advantages over agonists is the immediate suppression of intrinsic endocrine activity, without an initial surge in hormone levels. In addition, the overall duration of stimulation is usually reduced and less intense stimulation of the ovaries is required. These drugs are prescribed either once in a dose of 3 mg or from the 7-8th day of the cycle (with an average follicle diameter of 12-14 mm) in the form of subcutaneous injections (0.25 mg) for several days.
Selecting the right protocol
The choice of stimulation protocol depends entirely on the FSH reading, the LH to FSH ratio and the type of ovary. You also need to take into account age and increased body weight when prescribing a puncture. Excessive weight gives a weak ovarian response to stimulation, while very low weight, on the contrary, can cause high degree of hyperstimulation. Initial doses of FSH should be prescribed depending on BMI (body weight index).
1. Stimulation with clostilbegit (Clomid, Serophene, Clomiphene citrate).
Classically, clostilbegit is prescribed in a dose of 1-3 tablets (50 mg each) per day from days 5 to 9 of the cycle. To ensure ovulation, the drug hCG (pregnyl, prophase, choragon) can be prescribed when the follicle reaches a size of 18-24 mm. In support, estrogen-containing drugs (Progynova, Divigel, Estrogel) are often prescribed from 5 to 21 dc.
2. Protocols with gonadotropins.
To obtain a larger number of cells than when using clostilbegit, preparations of human menopausal or recombinant gonadotropin are used. These drugs begin to be administered in the form of subcutaneous or intramuscular injections, usually on the 2-3rd day of the menstrual cycle. Classically, stimulation is continued until the dominant follicles reach a diameter of 18 mm. After this, hCG drugs are prescribed.
Examples of possible protocol options:
• Treatment begins on the 2nd day at a dosage of 150 IU FSH or HMG per day. On days 8-9 of the cycle, the ovarian response is monitored. If the diameter of the follicles reaches 12 mm, then continue in the same mode. If the ovarian response is lower than expected, then increase the dose to 225 IU per day (3 ampoules of the drug, 75 IU each). The next control is carried out on days 11-12 of the cycle and, depending on the result, the dosage is increased or the same regimen is left. The hCG drug is prescribed when the diameter of the largest follicle reaches 18-24 mm.
• Stimulation begins at 250-300 IU. When the maximum follicle reaches a diameter of 12 mm, gradually reduce the dose every 3 days until hCG is administered. This protocol may be recommended for patients with polycystic ovary syndrome.
• Protocol to simulate the natural menstrual cycle. Stimulation begins on day 3 of the cycle with dosages of 75 – 150 IU. The dosage was gradually increased until the leading follicle reached 14 mm in diameter. After this, the drug load on the ovaries was gradually reduced until the day of hCG administration. This protocol requires a relatively small number of ampoules per stimulation, and also reduces the likelihood of developing ovarian hyperstimulation syndrome.
Important Notes:
1. Stimulation cannot be carried out in the presence of liquid formations d more than 12 mm and cysts of various etiologies.
2. When carrying out ovulation stimulation, ultrasound monitoring is required: before the start of stimulation and then every 2-3 days until the formation of VT.
3. In stimulated cycles, support of the second phase with progesterone drugs (utrozhestan, duphaston) is mandatory.
Source: https://www.babyplan.ru/forums/topic/51270-stimulyatsiya-ovulyatsii/#ixzz2to77nzgT
Indications for use
Ortilia is recommended for the following diseases:
- andexide,
- infertility,
- mastopathy,
- amenorrhea,
- menstrual irregularities,
- fibroma,
- andexit,
- endometriosis,
- the initial stage of adhesions in the pelvic area,
- disturbances in the functioning of the ovaries.
Various female diseases cause an excess or deficiency of certain hormones.
Progesterone plays an important role in pregnancy.
The boron uterus for conception is used to eliminate possible disorders by stimulating the production of the required amount of biologically active substances.
The saponin contained in the drug causes the mucus that covers the wall of the main organ to liquefy.
As a result, an egg is released, ready for fertilization.
The herbal tincture is also used for cystitis, gastritis, enuresis, kidney disease, diabetes, rheumatism, enterocolitis, and gout. It can additionally be used to improve the functioning of the endocrine system, enhance immunity, and alleviate respiratory tract ailments.
Application
Many people are interested in how to drink boron uterus. It all depends on the type of medication and the disease being diagnosed. It has various forms:
- alcohol tinctures,
- drops,
- pills,
- decoctions,
- capsules,
- vaginal suppositories.
To prepare a decoction, pour 10 grams of herb with a scant of hot water. It will brew within an hour. It should be taken after meals three times a day, one teaspoon. It is this regimen that is prescribed for infertility.
If you need to eliminate inflammation, then 400 milligrams of water should be poured into 30 grams of dry grass. Brewing takes place for five minutes in a water bath. After this, the resulting mixture is passed through cheesecloth. Doctors recommend consuming a tablespoon of it 4 times a day.
An alcoholic version is also prepared independently. This requires 0.5 liters of vodka and 50 grams of grass. The tincture of the mixture of the above elements is aged for a month. By the way, when preparing decoctions, it is important to use glass or enamel dishes.









